A 70 year-old patient was in our office with complaints regarding his right hip and shoulder pain. Patient explained that she fell on ice in the parking lot at work and has been experiencing pain since. She is currently working as a NP for empire medical services.
The patient reported that lifting worsened the pain. For associated symptoms, she reported pain with motion but reports no weakness, no numbness, no tingling, no swelling, no redness, no warmth, no ecchymosis, no catching/locking, no popping/clicking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness. For location, she reports right. For quality, she reports burning, stabbing, and frequent.
The patient presented an MRI result and showed complete tears of the supraspinatus and infraspinatus tendons with retraction as described. Subscapularis tendinosis with superimposed low-grade intrasubstance partial-thickness tear. Mild supraspinatus and infraspinatus muscle atrophy.
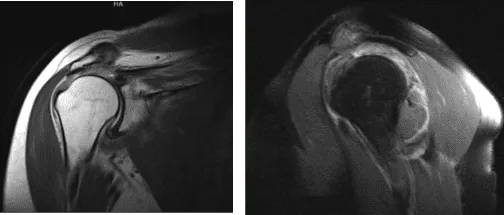
MRI right shoulder non-contrast
We discussed treatment options and tried physical therapy and conservative treatment for one month. The patient did not get better and agreed for surgical management.
We discussed the risks and benefits including infection, bleeding, partial repair, improper healing, failure of repair, and need for repeat surgery including need for reverse shoulder arthroscopy in future. We discussed rehabilitation. We also discussed systemic complications. The patient understood and signed informed consent.
The patient was taken to the operating room where she was placed on a well-padded operating table. General anesthesia was given. The patient was put in the left lateral position with the right shoulder up. Preoperative antibiotic was given. The patient was positioned with the use of a bean bag.
Axillary roll was inserted. All the bony sites were well padded. The right shoulder was prepped and draped aseptically in usual fashion. A posteroanterior portal was made to the soft spot into the glenohumeral joint. An antero anterior portal was made with the use of a spinal needle in the rotator interval.
A shaver was introduced from the anterior portal and scoped from the posterior portal. Examination showed fraying of the glenoid labrum, partial tearing of the subscapularis, partial tearing of the biceps, and large rotator cuff tear. Tenotomy of the biceps was done intra-articularly and the tendon was allowed to retract.
Debridement of the glenohumeral joint of the labrum as well as subscapularis was performed using the shaver. Now, the arthroscope was entered into the subacromial space. Shaver was introduced from the anterosuperior portal and bursa was debrided. Acromial spur was seen.
A large rotator cuff was present. The landmark on the rotator cuff was prepared using a burr. After the bursectomy and preparation, repair of the rotator cuff was performed using Arthrex triple-loaded anchors. Two sutures with four tails of both anchors were used to pass mattress sutures.
The sutures were tied on each other, which allowed rotator cuff repair. The rotator cuff was initially mobilized with the use of shaver and wand. It was retracted up to the level of the glenoid and was difficult to get. After the knots were done, the rotator cuff was satisfactorily repaired.
A trial for lateral load was performed, but could not be done due to the swelling in the bursa. Now, the thermal wand was used to do the subacromial decompression followed by burr to excise the subacromial spur. Distal clavicle excision was also performed using the burr for the posterior as well as anterior portal sequentially. Final pictures were taken and saved.
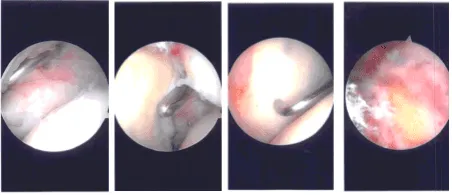
Intraoperative Arthroscopy Images
The scope was removed and the shoulder was irrigated and drained. Now, the traction was removed, and the shoulder was put in abduction and external rotation. Incision was given into the anterior port of axilla.
Skin, subcutaneous tissue, and fascia were cut in the line of incision. Interval was made along the inferior border of the pectoralis major and bicipital groove could be reached. The biceps tendon could be found and was extracted. Whipstitch suture was done using FiberLoop. Excess tendon was cut.
Anterior portal entry was marked for later use of Bovie and the Beath pin was drilled bicortically. Unicortical drilling for a 7 mm screw was also done. A button was loaded onto the tendon and was passed bicortically, flipped, and tightened.
The suture was passed onto the tendon and tied to each other following which the button was passed on one of the suture limbs and tightened over the tendon. At the end, the suture was passed through the tendon and tied onto each other.
Finding the repair satisfactory, the wound was thoroughly washed and drained. The closure was done in layers using 0-Vicryl, 2-0 Vicryl, and 3-0 Monocryl. Shoulder scope portals were closed using 3-0 nylon. The patient was given a brachial block before the surgery.
Wounds were dressed using Xeroform, 4 x 4, ABD, and paper tape. Shoulder immobilizer was applied after the surgery. The patient was extubated and moved to recovery in stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on her knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 22, 2025.
