Based on research, handball players who achieve high ball-throwing speed in handball require high shoulder internal and external muscle strength and power. Handball sports was said to be one of the playing contact games that exhibit aggression and takes place during executing offensive and defensive skills.
Patient presents shoulder & biceps pain from playing handball. He saw an increasing bulge of right biceps. He also presented his X-ray results, clearly showing the mild to moderate degenerative changes to the right acromioclavicular joint. By this time, we agreed to proceed with treatment options including Physical Therapy, Injection and MRI to identify the real condition of his shoulder.

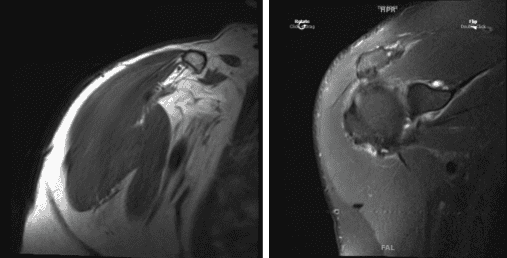
After a week, the patient presented his MRI. Impression as follows: Mild-moderate supraspinatus and infraspinatus tendinosis, with mild bursal fraying of junctional-zone fibers. Small, low-grade interstitial tear within the inferior subscapularis tendon.
Background mild-moderate subscapularis tendinosis, with low-grade intrasubstance fissuring superiorly. Complete versus near-complete rupture of the intra-articular segment of the biceps tendon, with retraction of the distal tendon stumps of the bicipital groove. Additional shortness and segment split tearing the extra-articular biceps tendon.
Short stump of the biceps anchor remains attached to the superior glenoid margin. Posterosuperior labral tearing (9-1:00, associated with a large Para labral cyst that tracks medially and anterosuperiorly; dominant cyst locule is situated anterior to the supraspinatus muscle. Moderate acromioclavicular joint arthrosis. Mild subacromial bursitis. Mild subacromial spurring.
We discussed treatment options and opted for surgical management. The patient had a trip to Hawaii after which when he came, he was not getting medically cleared due to hypertension. We could take the patient now at the earliest after all the medical clearances.
We discussed treatment options and discussed risks and complications including infection, bleeding, injury to adjacent nerves and vessels, failure, need for repeat surgery, and shoulder arthritis among others. We discussed systemic complications. The patient understood and signed an informed consent.
The patient was taken to the operating room where a supraclavicular block was given by the anesthesia team. The patient was intubated for general anesthesia. The patient was turned into the left lateral position with the right shoulder up.
The patient was placed in a semi-lateral position on a beanbag. All the bony prominences were well padded. The right shoulder was prepped and draped aseptically in the usual fashion. Time-out was called. Preop antibiotic was given.
A lateral posterior entry portal was made for the arthroscope. Arthroscope was inserted into the glenohumeral joint. Examination showed considerable fraying of the glenoid labrum with absent biceps tendon. There was fraying of the rotator cuff in the rotator interval as well as the subscapularis tendon.
Debridement of the subscapularis tendon and the glenoid labrum with a burr was performed through anterior and superior portals. Shaver was used. The labrum was also debrided. Pictures were taken and saved.
The arthroscope was inserted into the subacromial space where examination showed fraying and partial tearing of the supraspinatus and infraspinatus. Debridement was done with the use of a shaver. Impingement could be seen on the acromion, which was cleaned.
Coblation wand was used followed by a #6-0 burr to perform acromioplasty and release of coracoacromial ligament. There was arthritis in the AC joint. So, a distal clavicular excision was done with the use of burr and Coblation wand. A 0.5 cm of distal clavicle was excised.
First week post operative. He denies fever and chills and pain is in good control. Post Operative Exam: General Appearance: no swelling or warmth; tenderness, passive motion limited, and active motion limited; and wound clean and dry and neurovascular intact.
Four weeks post-operative. Patient not yet started physical therapy but said that the shoulder is ranging well. We agreed to go with conservative management for now.
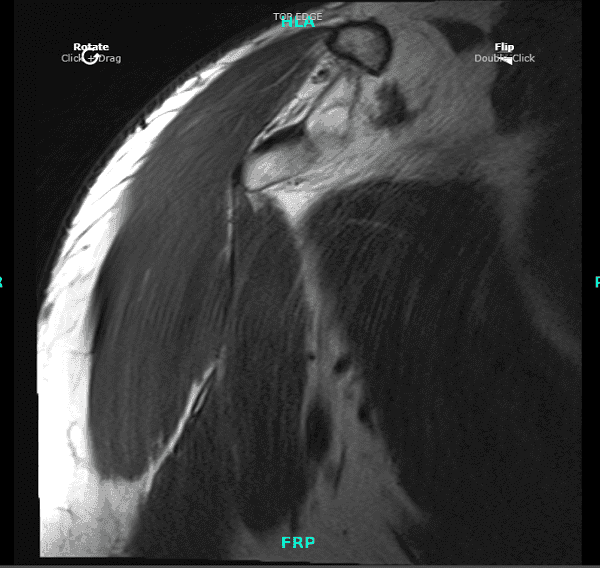
Eight weeks post operative. Patient started his PT and was doing well. We decided to have an MRI to see his shoulder condition. The MRI impression showed biceps tenodesis with surgical anchor/ endo button at the level of proximal humerus.
There is scar remodeling and heterogeneity of the tacked biceps tendon at the anchor, likely reflecting postsurgical changes. No high-grade or retracted fibers visualized.
The patient gets well after the surgery. With continuous follow up visits, conservative management and with the help of physical therapy. Patient able to return to his normal routine and play his sports handball after 2 months of recovery.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
