The patient is a 62-yr-old male, self-referred, with complaints of pain to bilateral knees Lt >> Rt since last year. The patient does not recall injuring himself. The patient had recently started running as an exercise and stated that the pain has significantly increased in intensity.
The pain is moderate to severe in intensity. The patient describes the pain as sharp. The pain is constant and does not disturb sleep. The pain is associated with swelling, crepitus, and giving way. The problem has been getting worse since and activities such as walking, standing, bending, squatting, kneeling, stairs make the symptoms worse. Rest makes the symptoms better. The Patient has not undergone surgery for the symptoms.
The patient is a truck driver by profession and his medical history is significant for hypertension, asthma, and hyperlipidemia. He is currently taking hydrochlorothiazide, Symbicort inhaler, and Lipitor. He denies any known drug allergies. The patient is a non-smoker.
On examination of the left knee, the patient is tender to palpation along the medial joint line and has mild effusion. The patient also has patellofemoral crepitus and tenderness on palpation along the medial and lateral patellofemoral joint line. The patellar grinding test is positive.
The patient has discomfort with McMurray’s maneuvers, and the knee is stable. The knee lacked full flexion secondary to the effusion but had full extension. They have 5/5 strength and are neurovascularly intact distally. There are no erythema, warmth, or skin lesions present.
On examination of the contralateral extremity, the patient is nontender to palpation and has an excellent range of motion, stability, and strength.
MRI of the left knee suggested a complex tear of the body and posterior horn the medial meniscus. Moderate patellofemoral chondromalacia associated moderate-sized joint effusion and capsular inflammation.
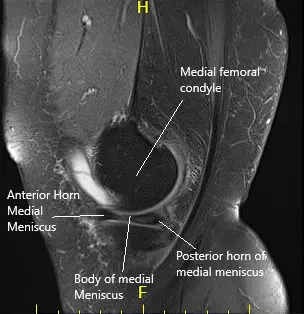
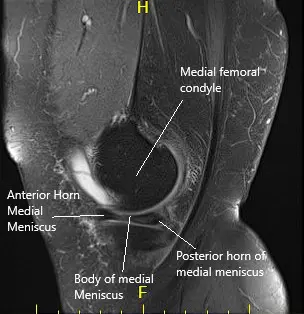
MRI of the left knee in sagittal and coronal sections.
We discussed treatment options and the patient opted for surgical management. We discussed risks, benefits, and complications of the treatment. The risks, benefits, alternatives, and complications were discussed with the patient at length. We discussed infection, bleeding, injury to nerves and vessels, knee pain, swelling, the progression of arthritis, the need for cortisone injections in the future and the need for rehabilitation. The patient understood and signed informed consent.
A lateral entry portal was made. The scope was entered and the knee was examined. There was patellofemoral arthritis. The scope was entered into the medial compartment. A medial entry portal was made using a spinal needle.
The medial meniscus was examined and found to have its margin fraying in the margin as well as degeneration of the inferior surface of the posterior horn of the medial meniscus.
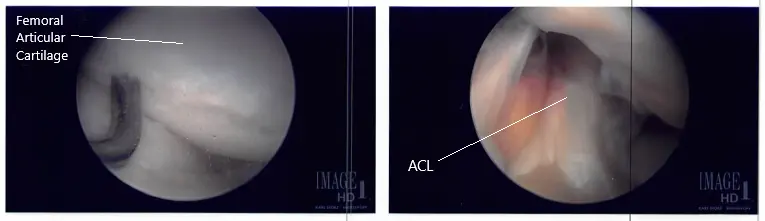
The shaver was used to remove all the fraying and balance the meniscus. The scope was entered into the intertrochlear notch, where ACL was found to be intact. The scope was introduced into the lateral compartment, where lateral meniscus was also found to be intact. There was stage II to stage III arthritis of the medial femoral condyle, which was cleaned using a shaver. There was no chondral damage to the lateral femoral condyle.

Intraoperative arthroscope images.
The scope was entered into the patellofemoral joint, where there was grade III to grade IV arthritis and over the trochlea, grade I to grade II over the posterior surface of the patella. Shaver and punch were used to remove all the loose cartilage from the trochlea as well as the patella. The cartilage was balanced to a stable margin. The knee was again examined and found to be adequately debrided.
Intraoperative arthroscope images.
The knee was copiously irrigated with normal saline. Final images were saved. The scope was removed and the incision was closed using #4-0 nylon. An 18 cc of Depo-Medrol mixed with 6 ccs of 0.5% Marcaine was introduced into the knee joint. The dressing was done. Tourniquet was removed. The patient was extubated and moved to the postoperative care unit in stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on March 20, 2026.