The patient is a 48-year-old art teacher who complains of left shoulder pain for the past year. The pain is located deep inside the shoulder and recently the patient has been waking up at night secondary to pain. The pain used to initially get better with Tylenol but she has had no relief with pain medications in the last month.
The patient denies any injury or fall precipitating the symptoms. Activities such as that involve overhead movement of the shoulder such as combing hair, lifting, shower, driving make the symptoms worse. The pain is reported to be sharp at night that wakes her up and is unrelenting despite using pain medications. She states she is unable to work secondary to pain.
The patient tried conservative management without any relief. She had a trial of medications, cortisone injections, and physical therapy. The patient reports the pain as a significant deterrent to her day-to-day activities. Her medical history is significant for chronic kidney disease, hypertension, and asthma.
Her current medications include lisinopril, spironolactone, amlodipine, and inhaled albuterol as needed. Her surgical history is significant for the repair of a femoral hernia five years ago.
MRI image of the left shoulder showing a complete tear of the rotator cuff.
The physical examination of the left shoulder revealed tenderness of the greater tuberosity and the bicipital groove. There is also tenderness to palpation at the subacromial bursa and the pectoralis major insertion. The range of motion of the left shoulder: forward flexion (160 deg.), extension (30 deg.), external rotation at 0 deg. of abduction (50 deg.), and abduction (160 deg.). Hawkin’s test, Empty Cans sign, and Neer’s impingement tests are positive.
Radiological studies of the left shoulder suggested a complete tear of the supraspinatus tendon with 8 mm of medial retraction, infraspinatus, and long head biceps tendinosis, subacromial/subdeltoid, and subcoracoid bursitis, AC arthrosis, and degeneration of the superior posterior superior labrum.
Various treatment options were discussed with the patient and the patient opted for surgical management. Risks and benefits including infection, bleeding, nonhealing, repeat surgery, injury to adjacent nerves and vessels, rehabilitation and stiffness, need for manipulation among others were discussed with the patient. The patient understood and signed the informed consent.
PREOPERATIVE DIAGNOSES:
- Rotator cuff tear of the left shoulder.
- AC arthritis of the left shoulder.
- Type 2 acromion of the left shoulder.
- Biceps tendonitis of the left shoulder.
POSTOPERATIVE DIAGNOSES:
- Complete rotator cuff tear of the supraspinatus and infraspinatus of the left shoulder.
- AC arthritis, left shoulder.
- Acromial spur and type 2 acromion, left shoulder.
OPERATIONS:
- Left shoulder arthroscopic rotator cuff repair (double row).
- Arthroscopic left shoulder limited debridement.
- Left shoulder arthroscopic acromioplasty and subacromial decompression.
- Left shoulder arthroscopic distal clavicle excision.
DESCRIPTION OF PROCEDURE: The patient was taken to the operating room where a supraclavicular block was given. General anesthesia was induced. The patient was turned into the right lateral position with the left shoulder up. The axillary roll was put in place. A Bean bag was used for positioning. All the bony prominences were well padded. The left upper extremity was prepped and draped aseptically in the usual fashion. Preoperative antibiotics were given in the form of Ancef 2 g. Time-out was called.
The posterior entry portal for the shoulder was made and the scope was entered into the glenohumeral joint. Entry to the anterior portal was made using a spinal needle through the rotator interval and a cannula was inserted. The probe was used by examining the shoulder and found to have mild osteoarthritis, grade 1 to grade 2 osteoarthritis of the glenoid surface center.
There was partial tearing of the superior subscapularis, which was debrided. There was mild tendinitis of the biceps tendon but no tears and nothing was done for that. Complete rotator cuff tear was seen in the supraspinatus and infraspinatus of the shoulder. There was fraying of the glenoid labrum, which was debrided using the shaver. The rest of the examination of the shoulder was normal.
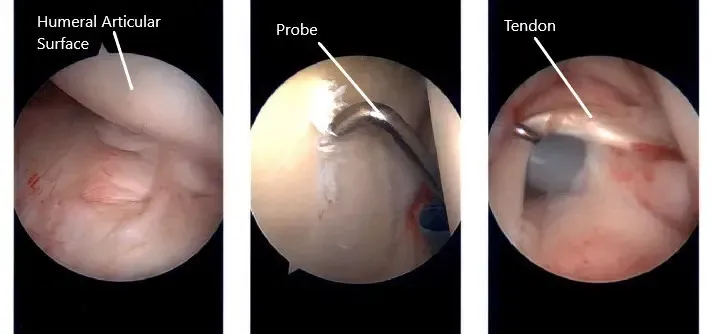
Intraoperative arthroscopic images of the left shoulder.
The scope was entered through the anterior portal, to confirm the findings. Now, the scope was entered into the subacromial space. Examination showed bursitis, which was debrided using the shaver. A big tear of the supraspinatus and infraspinatus was found.
The tear was extending up to the biceps tendon. Acromioplasty was performed with the use of a Coblation thermal wand followed by a burr. The anterior acromial spur was removed as well as CA ligament was released.
Now the focus was moved to the tear. A lateral portal was made with the help of a spinal needle and a shaver was introduced followed by decortication of bone for healing. Two Healicoil regenesorb anchors 4.75mm Smith and Nephew anchors were used for the repair. Four tails of the two anchors were passed through the rotator cuff from anterior to posterior avoiding the biceps tendon.
A good approximation of the rotator cuff was achieved with knots medially. The lateral row was planned and marked. The suture threads were all retrieved from the lateral portal and lateral row fixation was done using the Helicoil knotless anchor 5.0 from Smith & Nephew after satisfactory reduction and fixation of the rotator cuff was achieved.
Now, the attention was focused on the AC joint, which was found to be arthritic. Debridement and excision of about 10mm of the distal end of the clavicle were done using burr from the posterior and followed by the anterior portal. Final pictures were taken of the distal clavicle and the acromioplasty as well as the rotator cuff repair.
The shoulder was thoroughly irrigated and drained. The closure was done using #3-0 nylon. The dressing was performed using ABD and tape. The left arm was put in a shoulder sling and the patient was extubated and moved to the recovery unit in a stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
