Acromioplasty is a surgical surgery that involves cutting away the acromion of the shoulder bone. It is designed to smooth the acromion bone (found on the shoulder blade), preventing the Supraspinatus tendon (part of the rotator cuff) from rubbing against it and providing relief from shoulder pain.
A 61 year-old female patient visits the office with complaints of pain in the left shoulder. Patient stated she was moving her dresser when she felt her shoulder pop. She is morbidly obese and has undergone a sleeve procedure in the past year. She also underwent RCR Rt side x 2, 2 years back with good results. She also complains of pain and swelling over the medial clavicle.
Upon the examination, considering pain and swelling over the medial clavicle that she is unable to carry out activities of daily living we agreed to do a stat MRI of her shoulder. Aside from this, the patient is Morbid obesity (BMI – 55).
MRI Clavicle has been done and presented in the office. Acromion and bursa: The acromion has a curved configuration (type II). Moderate degenerative changes are present at the acromioclavicular joint. A small amount of fluid is present in the subacromial/subdeltoid bursa.
Rotator cuff tendons: Supraspinatus tendinosis present with high-grade partial-thickness articular sided tearing and a full-thickness component involving the anterior 2.2 cm of the distal supraspinatus tendon.
Infraspinatus tendinosis is present with high-grade partial-thickness articular sided tearing. Subscapularis tendinosis is also present with partial tearing at its insertion. Biceps tendons: There is no visualization of the long head of the biceps tendon, consistent with a complete tear and distal retraction.
Cartilage and labrum: Superficial cartilage irregularity is present in the glenohumeral joint. Degenerative tearing of the posterosuperior glenoid labrum is present. Bone marrow:
Subchondral cyst formation is present on the posterior aspect of the greater tuberosity. The bone marrow signal is overall age appropriate.
There is no evidence for significant lymphadenopathy in the visualized portions of the axilla. No asymmetric rotator cuff muscle atrophy is present. We decided to do another MRI to run more tests about her shoulder.
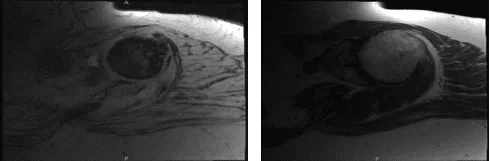
MRI first result
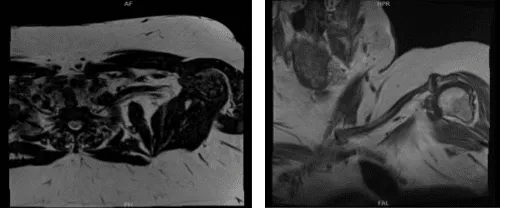
MRI second result
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections and surgical options. We also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
We also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. We talked about the possibility of not being able to alleviate all of the discomfort.
Ample time was given to decide, we have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome and post operative protocol. The patient has understood and expressed her desire to proceed with surgery and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. The patient was put in the right lateral position with the left shoulder up. Left shoulder was prepped and draped aseptically and put abduction and flexion. Time-out was called.
Preop antibiotic in the form of clindamycin was given. A posterior entry portal was made and shoulder scope was inserted through the glenohumeral joint. Examination of the joint showed absence of biceps. There was degeneration of the labrum as well as the subscapularis muscle. Debridement was done. Rotator cuff tears could be seen.
After a thorough examination and debridement of the shoulder, glenohumeral joint, the scope was inserted into the subacromial space. Subacromial bursectomy was performed. Acromioplasty was performed and there was lateral as well as anterior edge acromial spur which was removed.
CA ligament was released. The AC joint was normal and decided not to be done. Large rotator cuff would be seen. Preparation of rotator cuff tear was done. A bunch of owls were used for preparation of the anchor. The bone was soft.
Two anchors were used and all the four sutures were passed through the rotator cuff edges and tied over each other. Partial reduction of the tear was achieved. A third anchor was again used to augment the repair.
Lateral row was attempted but because of the poor bone quality, this one would not hold and was aborted. Final pictures were taken and saved. The shoulder was thoroughly cleaned and closed using nylon. The patient was extubated and moved to recovery in stable condition. Shoulder immobilizer was applied.
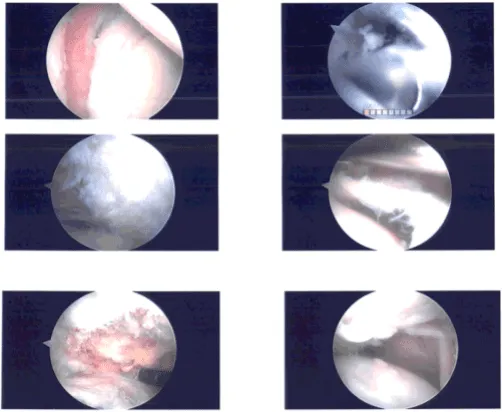
Intraoperative photo
Two weeks after the surgery, we removed the stitches. We have decided to proceed with a home exercise program for rehabilitation of the shoulder and continue with ice and elevation of the shoulder to decrease swelling and pain.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications. We also discussed to the patient the risk and benefits and common side effects of taking these medications.
After a month, the patient visits the office for follow up checkup, the patient is doing well, her pain is well controlled and she denies chills and fever. She is also about to start physical therapy for shoulder and take OTC anti-inflammatory medicine. The patient visits the office in three weeks’ time to evaluate her progress.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
