Patient is in our office with complaints of left ankle pain for over a week now. The patient remembers his injury in a motor vehicle accident. The pain is severe. Patient describes the pain as sharp, aching. The pain is constant and does disturb my sleep. The problem has been unchanged since it started.
Walking, standing, stairs, sitting make the symptoms worse while rest, heat, ice, lying down, bending forwards makes the symptoms better. Patient is currently working for Con Edison.
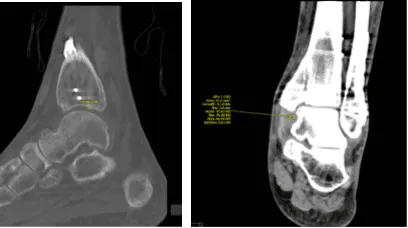
Patient presented his CT result and discussed it. Result showed Tri malleolar fracture on his left ankle. We discussed the treatment options for the patient’s diagnosis, which included: living with the extremity as it is, organized exercises, medicines, injections and surgical options.
We also discussed the nature and purpose of the treatment options along with the expected risks and benefits. The patient has expressed a desire to proceed with surgery, and I think that is a reasonable option.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to: anesthesia, infection, damage to nerves and blood vessels, blood loss, blood clots, and even death were discussed at length.
We also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
We talked about the possibility of not being able to alleviate all of the discomfort. Also, I explained there is no guarantee all the function and strength will return. The patient also understands the risks of failure to heal.
The patient understands implants may be utilized during this surgery. The patient expressed understanding of these risks and has elected to proceed with surgery.
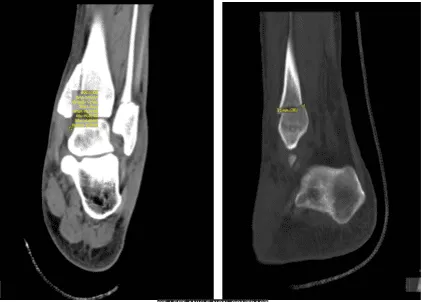
CT-Left ankle non-contrast
The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was induced. His left lower extremity was prepped and draped aseptically in a usual fashion after application of tourniquet on the thigh. A time-out was called.
Lateral distal fibular incision was given. The wound was exposed. The fracture site was opened. The fracture was thoroughly washed and cleaned. The fracture was reduced and held with a lateral pointed reduction clamp. The reduction was very good. distal fibular plate four-hole was used.
It was fixed using a combination of locking and nonlocking screws. The final fixation of distal fibula was checked on the C-arm and found to be adequate. Now, medial incision was given along the anteromedial distal tibia. The fracture was not opened this time. The fracture was well reduced by manipulation.
The ankle mortise was well formed. It was decided to fix it with a neutralizing plate and compression screws. A four-hole distal fibular plate was used and which was well aligned over the medial malleolus and distal tibia.
Two screws were passed across the fracture site from the distal fibular holes, nonlocking screws which achieved good compression on the fracture site. The neutralization part of the plate was done using proximal two nonlocking screws and one distal locking screw.
Final fixation was checked under C-arm and found to be adequate. The final pictures were taken and saved. The wounds were thoroughly washed and irrigated.
The closure was done in layers using 2-0 Vicryl, 4-0 Monocryl. Dry dressing was done. Posterior splint was applied. The patient was extubated and moved to recovery in a stable condition.
For one-week post operative checkup- he is doing well. Denies fever, chills, injury. He is in the Posterior splint. He is NWB with crutches. General Appearance showed no swelling, tenderness, or warmth and wound clean and dry, appropriate range of motion, and neurovascular intact.
By this time advised the patient to do the R.I.C.E Practice (Rest, Ice, Compression, and Elevation). Left ankle X Ray were reviewed and monitored for 32 weeks post-operative, it showed surgically treated fractures of the distal fibula and medial malleolus.
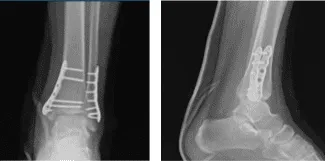
Left Ankle X-ray complete 3 or more views 1 week post operative
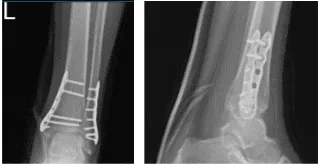
Left Ankle X-ray complete 3 or more views-4 week post operative

Left Ankle X-ray complete 3 or more views 8 weeks post operative
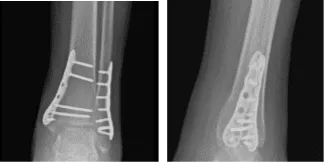
Left Ankle X-ray complete 3 or more views 16 weeks post operative
Left Ankle X-ray complete 3 or more views 8 months post operative
After 32 weeks postoperative the patient returned to the office and he is doing well. Denies fever, chills, injury. He is wearing regular shoes. He is FWB without support. He is having mild discomfort around the ankle. He is here for the left ankle follow up.
For further review of ankle condition, we agreed to take CT. Result showed healed Tri malleolar fracture status post ORIF with plate and screws in the fibula and the medial malleolus with mild deformity with 1 mm step off at the articular surface in the tibial plafond medially.
Mild deformity in the anterior margin of the tibial plafond. No new fractures. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. Patients regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
CT-Left ankle non-contrast
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
