Knee pain may be a result of an injury and medical conditions such as arthritis, gout and infections that affect people of all ages. Some knee pains respond well to self-care measures. Physical therapy and knee braces help to relieve pain. In some cases, surgical repair is required.
A 50-year old man with complaints of left knee pain visited our office. He remembers an injury in a fall, that he cannot put pressure on his knee. He also states that he feels a gap between the knee cap.
The pain is extremely severe in intensity and constant. The problem has been getting worse since it started. He takes Ibuprofen and puts ice on his knee to make the symptoms better.
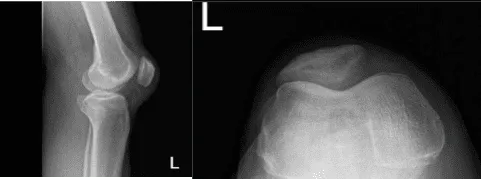
He was physically examined and an MRI was performed, which showed a complete tear of the quadriceps along with lateral meniscus tear, and partial tear of the ACL. The patient came to the emergency room due to intractable pain. We discussed treatment options and the patient opted for surgical management.
We discussed the risks of infection, bleeding, injury to adjacent nerves and vessels, need for repair, need for repair of the ACL, possible arthritic changes in the knee which needs debridement, future knee pain, need for steroid injections in case there is arthritis in the knee, rupture of the quadriceps again, need for repeat surgery, need for rehabilitation and possible knee stiffness in the future among others.
The patient understood the risks and benefits and complications well and signed an informed consent.

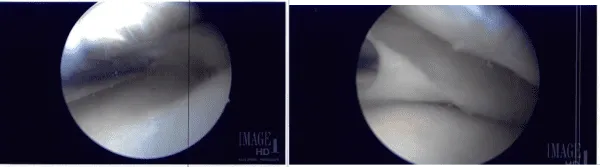
The patient underwent arthroscopic surgery. The procedures conducted were partial lateral meniscectomy, chondroplasty, ACL debridement and open repair of the quadriceps of the left knee. A left lateral entry portal was made and the scope was entered.
The knee was lavage with a lot of fluid to clean up the blood. visualization was not proper to the blood. The scope was moved to the medial tibiofemoral compartment. The medial meniscus was intact. There was no chondral damage. The scope was moved to the intercondylar area where partial ACL tear of the lateral side was found.
The debridement was done. The rest of the 90% of ACL was intact. The scope was moved to the lateral tibiofemoral compartment where the tear of the medial edge of the lateral meniscus was present. The tear was cleaned using right-sided biters and shavers. The rest of the lateral meniscus was intact. There was no chondral damage.
The scope was moved to the patellofemoral joint where trochlea grade 2 to grade 3 chondral damage was found. The chondral damage was debrided from the medial portal and followed by the lateral portal.
Copious lavage was performed. Arthroscopic pictures were taken and saved. The scope was removed. The knee was extended. The table was extended and a proper draping was performed. A midline vertical incision was put and centered over the superior pole of the patella.
The quadriceps tendon was found to be completely ruptured. The tendon was debrided. The stump of the tendon was over and the patella was removed. The bone was decorticated to fresh bleeding margins. three trans osseous tunnels were made and a silk tie was put for future use.
Now, the tendon was sutured using #5 FiberWire with a Krackow stitch x2. The four tails of the #5 FiberWire were passed through the three tunnels into the patella. The lateral and medial FiberWires were tied on to each other and the knots were buried.
Proper repair was found. The lateral and the medial retinaculum was repaired using #2 FiberWire. After proper closure, the wound was again lavage. The closure of the skin was performed using Vicryl #2-0 and Monocryl #4-0.
The arthroscopic portals were closed using nylon #4-0. The dressing was performed using Steri-Strips, Adaptic, 4 x 4s, ABD, Webril, and Ace wrap. The tourniquet was removed. The patient was extubated and moved to the recovery unit in a stable condition.
A week after surgery, the patient came for a follow up check-up. He is doing well and using the ROM knee brace. He denies having fever and chills. He was advised to undergo physical therapy, cold compress and take NSAIDs for pain management.
After that, he regularly went to the office every month for the follow up. He continued doing physical therapy until he fully recovered.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
