The patient is a 54-year-old male presenting with a complaint of right knee pain which has progressively worsened over the past 3 months. The pain first started a year ago without any precipitating event such as a fall or accident. The pain is described as sharp and is located on the outer aspect of the right knee.
The pain is severe in intensity and gets worse with activities such as walking, turning, twisting, navigating stairs. The patient tried physical therapy and medications for the past year but without any significant relief. The patient is a former smoker with a history of 25 pack years. The patient denies any use of illicit drugs.
The patient’s medical history is remarkable for hypothyroidism and osteoporosis. He is currently on levothyroxine, calcium, and vitamin D supplementation. The patient works as a business analyst and is currently not working secondary to pain. The patient walks with an antalgic gait with a decreased stance phase on the right. The patient currently uses a cane as an assistive device for ambulation.
On physical examination of the right knee, there is tenderness to palpation over the lateral femoral condyle. The range of motion was limited with flexion (150 deg), extension (10 deg.), and pain at extreme limits of the range. The Mcmurray’s and Apley’s compression tests were positive.

Intraoperative fluoroscopic image of the right knee showing tricalcium phosphate bone injection.
MRI of the right knee suggested extensive subchondral marrow edema at the lateral femoral condyle which may indicate a subchondral insufficiency trabecular microfracture. Various treatment options were discussed at length with the patient and the patient opted for surgical management.
The risks and benefits including infection, bleeding, nonhealing, need for repeat surgery, knee arthritis, need for rehabilitation, need for knee replacement in the future among others were discussed at length with the patient. The patient understood and signed the informed consent.
PREOPERATIVE DIAGNOSES:
- Lateral femoral condyle microfracture and subcondylar fractures.
POSTOPERATIVE DIAGNOSES:
- Lateral meniscus tear in the posterior root of the right knee.
- Osteochondral damage to the medial facet of the patella.
- Old osteochondral lesion of the medial facet of the patella.
- Microfracture and subcondylar fracture of the lateral femoral condyle.
OPERATION:
- Right knee arthroscopic lateral meniscectomy.
- Right knee arthroscopic chondroplasty of the medial femoral condyle as well as the medial facet of the patella.
- Arthroscopic-assisted percutaneous fixation of the lateral femoral condyle using tricalcium phosphate (subchondroplasty).
PROCEDURE: The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was induced. A tourniquet was applied. The preoperative antibiotic was given. The right lower extremity was prepped and draped aseptically in the usual fashion. Tourniquet was inflated. PF compartment showed osteoarthritic lesions of the medial facet of the patella. An arthroscope was entered into the medial compartment and a medial entry portal was made.
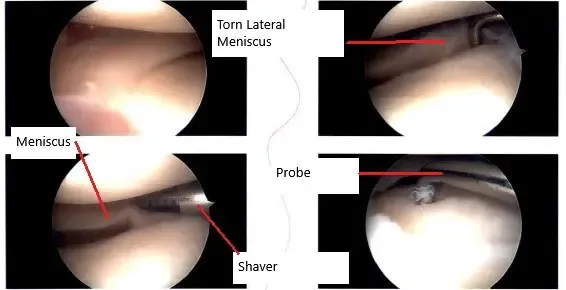
Intraoperative arthroscopic image showing the meniscus tear.
Examination of that medial compartment showed an old healed osteochondral lesion of the lateral surface of the medial femoral compartment which was stable. There was no tear of the medial meniscus. Examination of the intercondylar notch showed intact ACL. Examination of the lateral tibiofemoral compartment showed a tear of the posterior horn of the lateral meniscus. The lateral meniscus posterior horn was debrided using biters and shavers.
Examination of the patellofemoral compartment again shows an osteoarthritic lesion of the medial facet of the patella which was debrided using a shaver. The arthroscope was entered through the medial portal and findings were re-confirmed and final images were saved.
Now the focus was directed to the excision of the lateral femoral condyle. A fluoroscope was brought into the picture. Under guidance with fluoroscopy, a drill hole was made about 2.5 cm proximal and anterior to the inferior and posterior articular surface of the femoral condyle. It was inserted about 15 mm.
Another drill hole was made with a similar cannula about 0.5 cm proximal and anterior from the previous cannula directed posteriorly and inferiorly in the lateral femoral condyle. Pictures were taken in the AP and lateral view and found to be satisfactory.
Tricalcium phosphate bone cement was mixed and injected about 2.5 milliliters into each cannula and trochar was introduced. Pictures were taken in the C-arm and found cement to be into the bone only. An arthroscope was entered to examine the femoral condyle as well as the intercondylar notch and no bone cement could be seen extravasating there.
The knee scope was removed and the knee was drained completely. The cement was left to set. Once the bone cement was set for more than 12 minutes, the cannula was removed. The final picture was taken with the fluoroscope and saved. The knee was thoroughly drained and the wound was washed.
The closure was performed using #3-0 nylon; 9 ccs of 0.5% Naropin and 40 mg of Depo-Medrol were injected into the knee. The dressing was done using 4 x 4, ABD, Webril, and ACE wrap. The patient was to use crutches after the surgery. The patient was extubated and moved to recovery in a stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
