There are numerous different things that might cause bilateral shoulder pain. It can range from muscle tension or strain, which is typically brought on by bad posture or overuse, to trauma brought on by an injury.
To address shoulder issues like shoulder impingement and rotator cuff injuries, shoulder arthroscopy is a minimally invasive procedure. In most cases, the process is completed within an hour. In a few days, most people may return to their jobs or their studies. Recovery could take longer after more difficult operations.
A 65-year-old patient was in our office with complaints of bilateral shoulder pain left worse than right. The pain is severe in intensity and described the pain as sharp, dull, stabbing, throbbing, aching. The pain is intermittent and does disturb in sleep.
The pain is associated with numbness and tingling but is not associated with swelling, bruising, radiating pain, weakness, bowel or bladder abnormality, gait problem, giving way, or limping, hand function difficulty. The problem has been getting worse since it started.
Lifting makes the symptoms worse, however rest and ice makes the symptoms better. Patients have high cholesterol and high blood pressure. Patients do not smoke.
The patient is currently taking medication for cholesterol and blood pressure. Patient has had cortisone injections and PT in the past and has not had much relief.
Upon examination of the left and right shoulder, the patient sits with the scapula protracted and depressed. They are tender to palpation over the anterior supraspinatus and proximal biceps. There is mild palpable crepitus in the subacromial space with ranging.
The patient has restricted range of motion at the last 20 degrees of overhead abduction, and discomfort with above shoulder range of motion. The patient has discomfort with impingement maneuvers Whipple testing.
The shoulder is stable on exam. They have 5/5 strength and are neurovascularly intact distally. There are no erythema, warmth, or skin lesions present.
The patient presented MI results for her right shoulder and shown Intrasubstance tear anterior glenoid labmm. Partial tear rotator cuff distal supraspinatus tendon with adjacent lateral subdeltoid bursal effusion. Supraspinatus tendinopathy.
Acromioclavicular hypertrophic changes associated with impingement syndrome. MRI results for her left shoulder showed a partial tear rotator cuff undersurface proximal supraspinatus tendon. Distal supraspinatus tendinopathy. Acromioclavicular hypertrophic changes associated with impingement syndrome.
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections, and surgical options. We also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to anesthesia, infection, damage to nerves and blood vessels, blood loss, blood clots, and even death were discussed at length. We also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome.
The patient also understands there is a long rehabilitative process that typically follows the surgical procedure. We talked about the possibility of not being able to alleviate all of the discomfort. Also, I explained there is no guarantee all the function and strength will return. The patient also understands the risks of re-tear or failure to heal.
The patient understands implants may be utilized during this surgery. The patient expressed understanding of these risks and has elected to proceed with surgery. Ample time was given for questions, of which many were addressed. We have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome, and post operative protocol.
The patient was taken to the operating room where general anesthesia was induced. Supraclavicular block was performed before the intubation. The patient was put into lateral position along with a beanbag support, so that the right shoulder was up. The right shoulder was held in duction and prepped and draped aseptically in the usual fashion.
Preoperative antibiotic was given. The right shoulder was put into traction with weight. Entry portal was made posterolateral corner of acromion. The scope was entered into the glenohumeral joint. Examination of the glenohumeral joint was performed. There was grade 3 to grade 4 arthritis of the glenoid as well as the head of the humerus. There was fraying of the labrum.
The rotator cuff tear could be identified. Debridement of the subscapularis, labrum was performed. Debridement of head of the humerus was also performed.
Marking PDS suture was passed through the rotator cuff tear. Now the scope was entered into the subacromial space. There was extensive bursitis. Subacromial decompression was performed using a shaver.
There was fraying of the acromion W. along with a curved configuration (Type 2 acromion). The acromion was cleaned using a thermal wand followed by an acromioplasty with a bur.
The CA ligament was also released. After a thorough acromioplasty, the AC joint was examined and found to be degenerative. 1 cm of distal third clavicle” excision was also performed using a wand and followed by a bur.
About 1 cm of distal clavicle was excised. Now the rotator cuff tear was seen and cleaned. The footprint of rotator cuff was prepared. Accessory incisions were given for the lateral portal as well as posterosuperior portals for the insertion of the anchor. Smith & Nephew Healicoil peak anchor was used.
A two-tailed anchor was used and inserted into the head of the humerus. The tails were passed in a mattress suture pattern to the rotator cuff tear using FirstPass. The knots were tied.
The anterior knot was paired at medial row only. The posterior knot was put in a double- row repair using Smith & Nephew multifix anchor. Final pictures were taken.
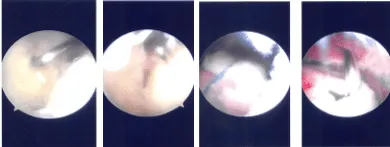
Intraoperative Arthroscopy Images
The shoulder was thoroughly washed and drained. The closure was performed using #4-0 nylon. The dressing was done using Adaptic, 4×4, ABD, and tape. The right lower extremity was put into an abduction pillow shoulder immobilizer. The patient was extubated and moved to the recovery in a stable condition.
The patient was seen for a post operative checkup. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation.
The patient did well after the surgery and continued physical therapy. Patient checked in for follow up visit after a month and seen significant improvement on her shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
