Patient is a 60 year-old male, who is here today with complaints of right shoulder and neck pain. He started experiencing the pain for over a year. The patient sustained the injury while being hit by a tractor trailer. Patient claims to have headaches. The pain is severe in intensity.
Patient describes the pain as sore and constant. The pain is associated with radiating pain into his arm, forearm and thumb. The problem has been getting worse since it started. Walking, standing, and bending make the symptoms worse. Rest makes the symptoms better.
Upon examination of the cervical spine, the patient is tender to palpation over the paraspinal musculature. They are nontender over the spinous processes and have no crepitus with range. There is limited range of motion of the spine due to discomfort. They have a negative Spurling’s test.
They sit with the scapular protracted and depressed. They are tender to palpation over the trapezius and rhomboids. They are nontender to palpation over the clavicle and elbow. There is no soft tissue swelling or ecchymosis.
The patient has a full range of motion of the shoulders. The shoulders are stable on exams. They have 5/5 strength, and are neurovascularly intact distally. There is no erythema, warmth, or skin lesions present.
Upon examination of the right shoulder, the patient sits with the scapula protracted and depressed. They are tender to palpation over the anterior supraspinatus and proximal biceps. There is mild palpable crepitus in the subacromial space with ranging.
The patient has restricted range of motion at the last 20 degrees of overhead abduction, and discomfort with above shoulder range of motion. The patient has discomfort with impingement maneuvers Whipple testing. The shoulder is stable on exams. They have 5/5 strength, and are neurovascularly intact distally. There is no erythema, warmth or skin lesions present.
X-ray of my right shoulder were presented. Right shoulder showed calcific tendinitis. Narrowing of the glenohumeral joint as well as the acromiohumeral space. Degenerative changes of the acromioclavicular joint. MRI of the right shoulder recommended.
MRI results showed a significant reason for pain- Infraspinatus calcific tendinitis. Rotator cuff tendinosis and a moderate partial-thickness bursal surface tear of the supraspinatus tendon with intermixed attenuation tissue.
Mild partial-thickness articular surface tear of the subscapularis tendon. Moderate AC joint arthrosis and focal tear of the superior labrum at the chondrolabral junction were also found.
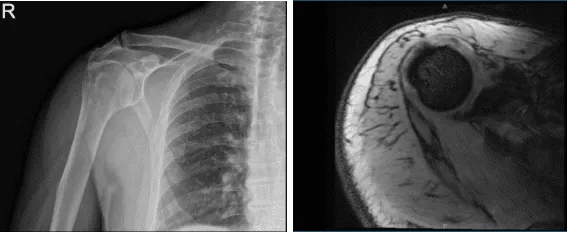
MRI X-ray of right shoulder
We discussed surgical and non-surgical treatment, but will think about the surgery and will proceed to elevation treatment for now and decided to receive cortisone injection.
After 4 weeks from the last visit, the patient came in again and complained about the same pain. Cortisone injection has not helped him in the past. Patient opted to do the surgery. Risk and benefits are discussed including the infection, bleeding, non-healing, repeat surgery and injury to adjacent nerves and vessels among others. The patient understood and signed informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. Preoperative antibiotic was given. The patient was turned in the left lateral position with the right shoulder up.
Bean Bag was inflated to hold him in incision. All the bony prominences were well padded. Right upper extremity was prepped and draped aseptically in the usual fashion. Time-out was called.
A posterior incision was given through the spot for the entry portal of the scope. The scope was entered into the glenohumeral joint and the glenohumeral joint was examined. There was labral tearing as well as articular site rotator cuff tearing. Debridement was performed using a shaver. Biceps were intact.
The subscapularis tendon as well as Inferior glenohumeral ligament and superior glenohumeral ligament were intact. There were grade 1 to grade 2 degenerative glenoid chondral changes using a shaver. Now, the scope was entered into the subacromial area where subacromial bursitis was present.
Shaver was used to decompress the subacromial region and bursectomy was performed. Acromial spurring and type 2 acromion were found. A burr was used to do the acromioplasty. The AC joint was found to be intact and no inflammation was found. The final pictures were taken.
The incision was closed with #3-0 nylon. Dressing was done using 4 x 4s, ABD, and tape. The patient was put in a shoulder sling and moved to recovery after extubating in stable condition.
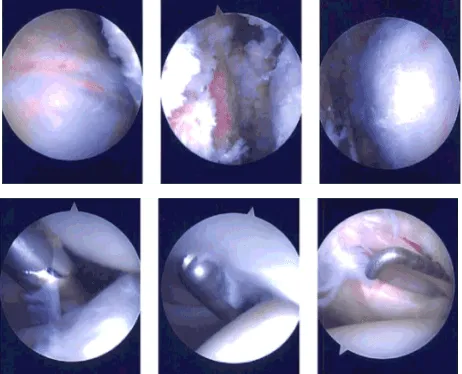
Intraoperative Arthroscopy Images
After a week post-operative, a patient came in. He has pain and swelling of the shoulder and redness around the incisions. He is in shoulder sling and is able to move the shoulder to some ROM. A month after the surgery, he denies tingling, numbness, weakness, radiating pain.
He decided to receive cortisone shots to ease the pain. After discussing the options for treatment and the risks of injection, the patient wished to proceed with the injection to reduce pain and swelling.
After a sterile prep, 3cc of 1% ropivacaine, 3cc of 0.5% marcaine and 80mg of depo-medrol were injected into the right shoulder subacromial space. The patient tolerated the procedure well and there were no complications.
Post injection pain, blood sugar elevation, skin discoloration, fatty atrophy and the signs of infection were discussed in detail. Patients get well with consistent follow up visits and without attending Physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
