Our forearm is made up of radius and ulna. They are perfectly working together, if the other one is injured, the other one is affected. Human bones can be fractured in many different ways but there is one fracture that requires emergency surgery and that is open fracture.
Most people with fractures do very well if proper care was given. On this note, we will discuss open reduction and internal fixation performed to a patient in Henry’s approach.
Patient is here with complaints of a fracture in ulna and radius of his right arm. He was on a bicycle and was hit by a car; hit and run. He also has abrasions over the right knee and left hand which he is dressing and cleaning.
Suspected diagnosis: Fracture of shaft of radius and/or ulna. General Appearance: deformity and swelling and skin in-tact, neurovascular intact, capillary refill normal, pulses normal, normal sensation, no tenderness on palpation, and location: (right forearm). Constitutional well-developed, well nourished, and not in distress.
Patient opted for surgical management. We discussed treatment options and the patient had opted for surgical management.
We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, failure of implant, failure of fracture, need for repeat surgery, systemic complication including blood clot, cardiac, pulmonary, neurological complications including death.
We also discussed the use of higher liver enzymes and the need for refraining from Tylenol as well as other hepatic toxic medication. He was also asked to be a primary care physician.
The patient was taken to the operating room, where he was placed on a well-padded operating table. General anesthesia was induced. The right upper extremity was prepped and draped aseptically after application of tourniquet. Time-out was called. Preoperative antibiotic was given.
Tourniquet was inflated. Anterior incision was given for the radius approach through the modified Henry’s approach. Interval was made between the brachioradialis and flexor carpi radialis. Radial artery was seen and retracted laterally. The fracture site was reached and opened.
There was a subtle comminution The fracture was washed thoroughly. Reduction was done using clamps. The reduction was a little difficult considering the fracture was a little old. Once the reduction was held, an 8-hole plate was used. It was fixed using three holes distally and four holes proximally.
It was fixed using a combination of locking and nonlocking screws, achieving compression over two of his screws proximally. Once the radius was completed, then it was checked in the C-arm.
Attention was diverted to the ulnar fracture. Exposure of the ulna was done through the posterior approach over the ulna. The fracture was opened and washed. There was a comminution of the fracture and a loose fragment.
The fracture was reduced and the loose fragment could be put in place and the fracture was well reduced. The fracture was fixed using an 8-hole plate and the combination of locking and nonlocking screws. Three holes were used distally and four holes proximally. After the satisfactory reduction, the final picture was taken and saved.
The wound was thoroughly washed. Tourniquet was released and hemostasis achieved. Closure was done in layers using 2-0 Vicryl for subcutaneous and 3-0 Monocryl for subcutaneous closure. The wound was dressed with 4x8s. Webril was applied.
Long-arm splint was applied using Ace wrap. The patient was extubated and moved to recovery in a stable condition. From the 1st week to 36th weeks, we monitored the progress of patients by doing regular X Ray. And it showed significant changes from patient condition.
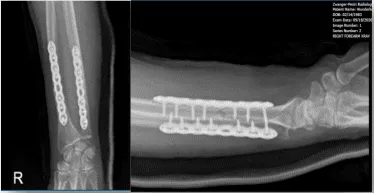
Right Forearm X-ray-1st week post-operative
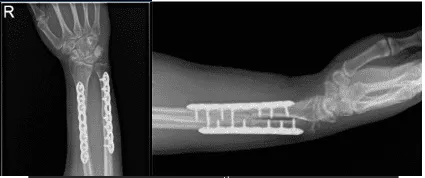
Right Forearm X-ray-16th week post-operative
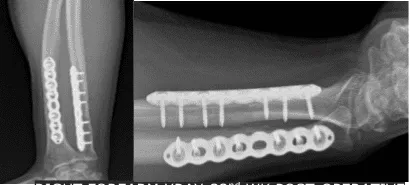
Right Forearm X-ray-32nd week post-operative
With consistent follow up visits, patients get well easily from his surgery. The patient tolerated activities and returned to his normal routine.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
