The optimum repair design should maximize the suture’s ability to fixate to bone, suture’s ability to fixate to tendon, suture’s resistance to abrasion, suture strength, knot and loop security, and restoration of the anatomic rotator cuff footprint (the region of bone to which the cuff tendons connect).
Any one of the shoulder bones might fracture, severely limiting your range of motion and producing excruciating agony. Injuries to the shoulder from falls, sports injuries, auto accidents, or other direct blows to the shoulder can result in shoulder fractures.
A 68 year-old patient visited our office with complaints regarding right shoulder pain. He also complains of lower back pain. After discussing the options for treatment and the risks of injection, the patient wished to proceed with the injection to reduce pain and swelling.
After a sterile prep, 3cc of 1% ropivacaine, 3cc of 0.5% marcaine and 80mg of depo-medrol were injected into the right shoulder subacromial space. The patient tolerated the procedure well and there were no complications. Post injection pain, blood sugar elevation, skin discoloration, fatty atrophy and the signs of infection were discussed in detail.
The patient presented MRI results that showed rotator cuff tendinosis most pronounced at supraspinatus tendon where a full-thickness tear at the central aspect of the insertion measures 8 mm and there is low-grade partial-thickness articular sided tearing extending more proximally into the critical zone.
Mild to moderate infraspinatus tendinosis with a small shallow articular sided tear. Small nondisplaced tear at the superior labrum. Tiny enchondroma within the humeral head.
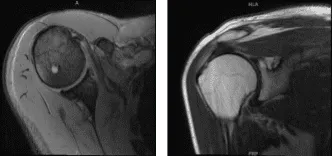
MRI Right shoulder non-contrast
We discussed surgical management and the complications including infection, bleeding, injury to nerves and vessels, shoulder rehabilitation, shoulder stiffness, development of arthritis in the future as the well as the need for shoulder replacement, failure of surgery and the need for repeat surgery, systemic complications including blood clots, cardiac, pulmonary complications among others.
The patient understood and signed informed consent. The patient was taken to the operating room where a supraclavicular block was secured.
The patient was sedated and placed in the left lateral position with the right shoulder up. All of the bony prominences were well-plated. The patient was placed in a bean bag.
The right shoulder was prepped and draped aseptically in the usual fashion. Preoperative antibiotic was given. An anterior portal was made through the posterior soft spot. The arthroscope was inserted.
An anterior superior portal made with the use of a spinal needle. Examination of the glenohumeral joint showed intact biceps. There was some scapularis tendon noted to be intact. There was a full thickness rotator cuff tear.
The arthroscope was inserted through the subacromial space where debridement of the subacromial space was entered with the use of a shaver. An acromioplasty was performed with the use of coblation wand to remove the acromial spur and make space for the repair.
The rotator cuff tear was débrided and the space was cleaned with the use of a bur. Triple plate cork screw anchor from Arthrex was used and inserted. The pigtails of the screws were passed sequentially from anterior to posterior in a horizontal mattress fashion.
All of the sutures were tied. Natural groove fixation was planned and achieved with the use of 4.75 SwiveLock naturally. Good repair was achieved. AC arthritis was seen and distal clavicle excision was done with the use of the bur by removal of 1 cm of the clavicle.
The shoulder was already cleared. Closure was done with the use of 3-0 nylon. Dressing was done with the use of Xeroform, 4 x4, ABD, tape. A shoulder immobilizer was applied. The patient was recovered and moved to the recovery room in stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
