The rotator cuff tendons are typically sewn back to the upper arm bone (humerus) during rotator cuff surgery, which is a significant procedure. Stiffness in that shoulder is the other main factor in patients’ pain following rotator cuff surgery.
Your doctor could advise arthroscopic surgery to repair the tear if you have a torn rotator cuff. A tiny camera called an arthroscope is inserted into your shoulder joint by the surgeon during an arthroscopic rotator cuff surgery.
The patient, an 18 year-old female went to the office with lower back, right shoulder, right hip and bilateral knee pain due to a car accident. She had no pain before the accident. She is doing PT at Caring hands.
X-rays were done and reviewed by the doctor; Osseous structures: there is no visible fracture or post fracture deformity. Bone mineralization appears normal. Joints: Joint spaces are preserved. High riding patella is seen bilaterally. Soft tissues: Unremarkable. With impression: Patella alta.
The patient had an MRI which showed a partial tear of the rotator cuff. We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, numbness, shoulder rehabilitation, shoulder stiffness, failure of surgery, and need for repeat surgery amongst others.
The patient understood and signed an informed consent. We also discussed systemic complications including blood clot, cardiac, pulmonary, and neurological complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where she was placed on a well-padded operating table. Supraclavicular block was given. General anesthesia was induced. The patient was put into the left lateral position with the right shoulder up. All the bony prominences were well padded.
The patient’s position was maintained in a beanbag. The right shoulder was prepped and draped aseptically in an usual fashion. The shoulder was put 45 degrees arm abduction and flexion on traction. Time-out was called. Preoperative tranexamic acid was given.
A posterior entry portal was made through a soft spot 1 cm inferior and posterior of the acromion. Arthroscope was inserted into the glenohumeral joint. Anterior portal was made with the use of a spinal needle and a probe was inserted through the cannula.
Examination of the glenohumeral joint showed no arthritis. Biceps were intact. The degenerative labrum was intact. The subscapularis tendon and supraspinatus tendon were intact. There was a partial high-grade tear of the infraspinatus tendon near the posterior part of the rotator interval.
Rest of the examination was intact. Spinal needle was used to pass the medial suture in the middle of the tear. The arthroscope was inserted in the subacromial region and the shaver was inserted through the anterior superior portal and subacromial bursa was excised with the use of shaver. There was no damage or spur on the acromion. The AC joint was intact and healthy.
Examination of the rotator cuff showed a soft spot along the infraspinatus which was debrided with the use of a shaver. The partial high-grade tear was converted into the complete tear. The plan was then to repair the tear.
Separate entry portals were made for the examination as well as insertion of the anchor. A # 4.75 Heallcoil Regenesorb four-tailed anchor was used from the Smith and Nephew and inserted into the head of the humerus after one suture of the anchor was passed through the anterior and the posterior margin and tied on to each other.
Satisfactory repair was achieved. Final pictures were taken and saved. The arthroscope was removed and the shoulder was irrigated and drained. Closure was done with the use of nylon # 3-0.
Dressing was done with the use of Adaptic, 4x8s, ABD, and tape. Shoulder immobilizer was applied. The patient was extubated and moved to the recovery unit in a stable condition.
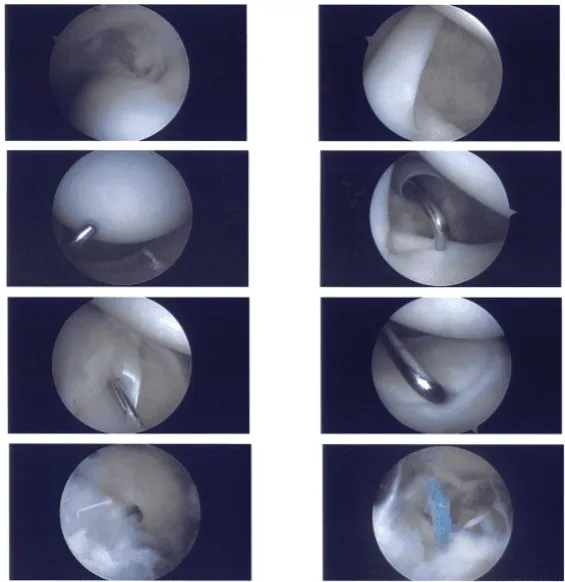
Intraoperative images
The patient is here today for her postoperative visit, no x-rays needed. She denies fever, chills. After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the shoulder.
We went over the arthroscopic pictures and removed the stitches during today’s visit. We will continue with ice and elevation of the shoulder to decrease swelling and pain.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications. We also discussed the risk and benefits and common side effects of taking these medications. The patient will be back in three weeks’ time to evaluate her progress.
After one month the patient was seen in the office for her postoperative visit, no x-rays needed. She has no fever and chills, so we agreed to go with conservative management for now. PT to be started, Ice/heat, Eeevation and taking OTC anti-inflammatory meds.
Follow up checkup every 4 weeks. With regular visits in the office and continued physical therapy, the patient did well after the surgery.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
