The surgeon will release the torn biceps tendon from the labrum during the biceps tenodesis operation. In some cases, the biceps tendon may be relocated to the upper arm bone (humerus). A surgeon can repair the biceps tendon using open or arthroscopic surgery.
Acromioplasty is a surgical technique that involves cutting away a portion of the acromion of the shoulder bone. The surgery is performed by surgeons to remove impingement of the rotator cuff tendon, which supports and strengthens the shoulder joint.
Acromioplasty is often referred to as subacromial decompression surgery. Acromioplasty, or acromion thinning, is routinely recommended for biceps tendonitis with subacromial impingement. Depending on the patient’s age and activity level, it is paired with a tenotomy or a biceps tenodesis.
The patient is a 54-year-old female who came into the office after falling and being unable to move her shoulder. She was in a lot of discomfort. The examination revealed a rotator cuff tear. An MRI revealed a significant rotator cuff tear in the left shoulder as well as a biceps subluxation.
We examined treatment alternatives and decided on surgical intervention. We reviewed risks and benefits such as infection, bleeding, nerve and vascular injury, failure of complete repair, failure of surgery, necessity for repeat surgery, and rehabilitation, among other things.
We also reviewed systemic concerns such as blood clots, cardiac, pulmonary, and neurological issues. The patient comprehended and signed an informed consent form.
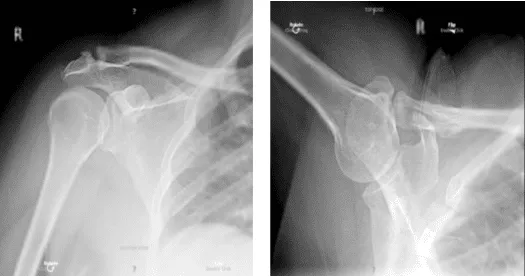
X-ray bilateral shoulders
The patient was brought to the operating room and placed on a well-padded operating table. The anesthesia department administered a supraclavicular block. The patient was put under general anesthesia and intubated. The patient was positioned right laterally, with the left shoulder raised.
All of the bony prominences were adequately cushioned. The patient was placed in a floppy lateral position using a beanbag. As usual, the left shoulder was prepared and draped aseptically. A timeout was issued. Landmarks were identified. A preoperative antibiotic was administered.
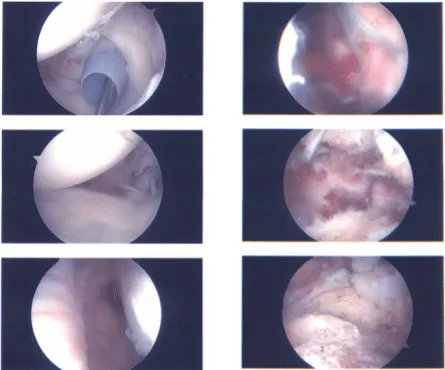
The posterior entry portal was created by cutting a soft area below the acromion’s posteroinferior edge. The arthroscope was introduced into the glenohumeral joint, where a significant rotator cuff tear, biceps subluxation, and partial subscapularis tearing could be noted.
A spinal needle was used to guide the anterosuperior boundary, and a shaver was used to debride the subscapularis tendon. The biceps stump was debrided, and the biceps tenotomy was performed. A subacromial bursectomy was conducted using an arthroscope placed in the subacromial region.
The big tear was visible. Each rotator cuff received two additional lateral portals from the anterolateral and posterolateral margins. An additional lateral portal was created for the anchor insertion. After debridement of the subacromial bursa, subacromial decompression and acromioplasty were performed using a coblation wand to provide a place for the repair.
A Speed Bridge was planned, and anterior and then posterior row anchors were placed. The anterior and posterior double loop sutures were used. To support the repair, two Fiber Loops were employed to tag the front and posterior margins.
A lateral row repair was planned, with one suture from each loop of the Speed Bridge from anterior to posterior, as well as the posterior tag posteriorly and the anterior tag anteriorly, which were dumped into the lateral tip of the humerus using SwiveLock x2.
A good double-row repair was accomplished. Because AC arthritis was present, the decision was made to do the distal clavicle resection. A centimeter of distal clavicle was excised using a coblation wand followed by a burr.
The shoulder was irrigated and drained carefully. Photographs were taken and preserved. The arthroscope was withdrawn, and the wounds were stitched up. An incision was made for about 3 cm into the anterior axillary fold, right below the pectoralis major tendon.
In the line of incision, the deltopectoral fascia was incised. To reach the bicipital groove, a finger was injected along the inferior margin of the pectoris between the pectoralis major and subscapularis. The bicipital tendon was found and extracted from the incision with difficulty using right-angle forceps.
A bovie was used to clear the bicipital groove. Baseball stitch sutures were placed roughly x5 around the musculotendinous junction in the biceps’ tendon. Biceps tendon excess was removed, and histology was performed.
An axillary roll was performed in the bicipital groove bicortically with a Beath pin, followed by reaming of the proximal cortex with a 6-mm drill. A bicortical vertical stitch was passed, reversed, and tightened. The stitch was then carried back through the tendon and sutured onto itself.
The suture was then removed via the EndoButton, and the EndoButton was reinserted and unicortically fastened to the biceps. To accomplish further fixation, the suture from the button was threaded into the tendon and knotted on itself. The wound was irrigated and drained carefully.
#0 Vicryl was used to close the fascia, #2-0 Vicryl in the subcutaneous tissue, and #3-0 Monocryl on the skin. Dressing was done with Xeroform, 4×4, ABD, and Bedford tape. In stable condition, the patient was placed in an abduction shoulder sling, extubated, and transported to recovery.
Intraoperative report
After one week the patient is here status post left shoulder arthroscopic rotator cuff repair for a post op visit. Patient’s pain is well controlled and she denies fever or chills. After examining treatment options, we chose to proceed with official physical therapy as well as a home exercise regimen for shoulder rehabilitation.
During the visit, we reviewed the arthroscopy images and removed the stitches. We will continue to use ice and elevate the shoulder to reduce swelling and pain. We will gradually wean them off any narcotic medications and transition them to anti-inflammatories and Tylenol as long as there are no contraindications.
We also covered the risks and benefits of taking these medications, as well as the most prevalent side effects. The patient will return in three weeks to assess their progress.
After three weeks the patient went back to the office for her post op visit. The patient’s pain is well controlled and she has denied fever or chills. Three months after the surgery, the patient visit the office for a post op visit.
Aside from the pain is well controlled and has no fever or chills. She is improving gradually with PT. The patient’s progress and development have been undeniable with continued physical treatment and regular attendance at his follow-up checkups.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 24, 2025.
