Acromioplasty is a surgical technique that includes cutting away a portion of the acromion of the shoulder bone. The surgery is performed by surgeons to remove impingement of the rotator cuff tendon, which supports and strengthens the shoulder joint.
Acromioplasty is often referred to as subacromial decompression surgery. At a long-term follow-up, patients who had rotator cuff repair with or without acromioplasty had better outcomes than before surgery.
The patient is a 22-year-old male who came into the office complaining of a right shoulder ache after an automobile accident. On evaluation, he was found to be feeble and to have a rotator cuff injury and impingement. We had an MRI, which revealed a tear in the right shoulder’s rotator cuff. There was acromial spurring as well as AC joint hypertrophy.
We spoke about our alternatives for care and decided to use surgery. Infection, hemorrhage, damage to nearby nerves and blood vessels, the need for more surgery, the need for rehabilitation, stiffness, and insufficient symptom relief were just a few of the dangers and advantages we covered. We also touched on systemic issues. The client was aware and gave informed consent.
The patient was transported to the operation room and given a supraclavicular block for sedation. General anesthesia was then administered. The patient was positioned on his left side. Axillary roll was added. All of the bony prominences were adequately cushioned.
To keep the patient in place, a bean bag was deflated. A preoperative antibiotic was administered. The right shoulder was prepared and draped aseptically as usual. The shoulder was placed on the traction pulley, which weighed 10 pounds. The shoulder was abducted and flexed. A timeout was issued.
An anterior portal was created for posterior entrance at the soft point. The arthroscope was implanted. The spinal needle was used to create an anterior and superior entrance hole. An examination of the shoulder joint revealed fraying of the anterior and posterior glenoid labrums.
The biceps were discovered to be completely intact. The rotator interval was fraying. Shaving revealed fraying of the labrum as well as the rotator interval. The cartilage was found to be undamaged.
The rotator cuff’s intra articular tear was nonexistent. The subacromial space was used to implant the arthroscope. The front of the probe was inserted. from the anterosuperior portal was inserted. There was a subacromial bursectomy.
Over the acromion’s underside, there were indications of impingement. Additionally, an infraspinatus partial tear was discovered. There was a debridement of the tear. The choice was made to use a medical rotation implant to heal the tear.
Additionally, the acromial spur was removed using a thermal wand and a bur. An acromioplasty was done. The AC joint was discovered to be in excellent form with no impingement.
Using a tiny rotation implant that was connected to the rotator cuff tendon using numerous screws, the decision was made not to repair a partial tear of the infraspinatus. Final images were captured and stored. It was irrigated and drained on the knee.
Nylon # 3-0 was used for the closure. The dressing materials used were tape, Xeroform, 4 x 4, and ABD. The patient’s shoulder was immobilized. The patient was transported to recovery in a stable state after being extubated.
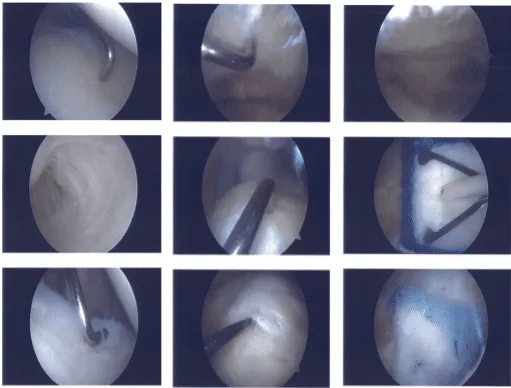
Clinical images
The patient went to the office for his one week post operative visit, no x-rays were needed and he has denied fever and chills. We chose to move through with official physical therapy as well as a home exercise program for shoulder rehabilitation after discussing our treatment choices.
During the visit, we took the sutures out. We’ll keep applying ice and elevating the shoulder to lessen pain and swelling. As long as there are no contraindications to these medications, we will wean them off of any narcotic medications before switching them to anti-inflammatories and Tylenol.
We also talked about the advantages, disadvantages, and typical adverse effects of using these medicines. In three weeks, the patient will return to assess their development.
No x-rays were required after one month for the patient who visited today for his post-operative appointment, and he denied fever and chills. He is receiving PT (Caring Hand) and is recuperating slowly. He is gradually weaning himself off the shoulder sling.
We discussed therapy alternatives such as PT, MRI, injection, and surgery. We agreed to use conservative management for the time being. PT will continue, as will the use of ice and elevation, as well as the use of over-the-counter anti-inflammatory medications.
After 4 weeks, there will be another checkup. Every time the patient visits the office, he demonstrates development and improves, even in slow progress.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
