Hip replacement is a useful surgery to treat hip pain. It involves us removing the worn-out, painful parts of your hip joint and replaces them with smooth artificial parts, so you can move without the pain and stiffness you had before.
Most people get this surgery because of arthritis that has not gotten better with rest, medicine, or physical therapy. This page focuses on the anterior approach, which means the surgeon reaches the hip from the front instead of the back or side. Going in from the front allows the surgeon move muscles aside instead of cutting through them This means less pain afterward and a faster recovery. Sometimes you can even go home the same day.
What condition does this surgery treat:
This surgery treats ongoing hip pain, most often caused by arthritis. Arthritis happens when the smooth cushioning inside your joint wears away This causes the bony ends of the joint to rub together and become inflamed. A few things can cause this:
Old childhood hip problems, trauma or infections that lead to pain years later.
Wear-and-tear arthritis (osteoarthritis): The most common condition as people get older. But younger people can get it from injuries or sports. Things like age, extra weight, family history, and an inactive lifestyle increase the risk.
Inflammatory arthritis: conditions like rheumatoid arthritis or psoriatic arthritis. Here the body mistakenly attacks its own joints resulting in damage over time. This also includes gout and pseudogout, which are caused by the accumulation of crystals in the joint. These can lead of chronic damage.
Loss of blood flow to the bone (called avascular necrosis), which slowly destroys the joint when it doesn’t get enough blood flow.
When do you need surgery:
Surgery is usually a last step, not a first one. Most people try non-surgical options first. This includes interventions such as losing weight, exercising, taking pain relievers like Tylenol or anti-inflammatory medicine, getting joint injections, doing physical therapy, or using a cane / walker.
If your hip still hurts after trying these interventions for several months, then we consider hip replacement surgery. It is considered a major operation. If your pain is bad enough to warrant a major operation, and you can commit to the months of rehabilitation, then surgery may be a good fit for you.
Hip replacement surgery can be done from the front (anterior), back (posterior) or side (lateral). All approached work to effectively treat arthritis related pain. However, anterior can has a quicker recovery early on.
At the three month mark, all patients are on similar footing. Not everyone is a candidate for the anterior approach of hip replacement. Large/obese/muscular patients are generally approached with more traditional approaches.
What happens during surgery:
You’ll be asleep or numbed from the waist down, lying on your back. The surgeon makes a cut about 4 to 6 inches long on the front of your hip and gently moves the muscles aside to reach the joint. Then they:
- Remove the damaged ball at the top of your thigh bone.
- Clean out the worn socket in your pelvis and fit in a new metal or ceramic cup, held in place with screws or a snug press-fit.
- Add a smooth durable plastic liner inside the cup so the joint glides easily.
- Place a metal stem into your thigh bone, held by either a tight fit or special bone cement.
- Attach a new metal or ceramic ball to the stem and fit it into the new socket.
- Close everything up in layers and put a clean dressing over the wound.
Surgeons sometimes use a live X-ray during the operation to place the new parts precisely. Good placement helps your legs stay even in length and helps the new hip last longer.
The images below show some of the implants that are used in the surgery:

Normal hip anatomy and position of femoral stem in hip replacement surgery.

Neutral Polyethylene Acetabular Liner
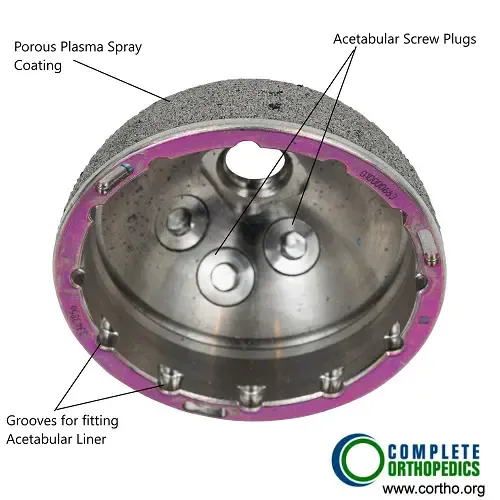
Acetabular Shell with screw holes and porous outer surface for bone ingrowth.
What does recovery look like:
Recovery from the front approach tends to be quicker because fewer muscles are disturbed. Once the anesthesia wears off, you can usually stand and walk with crutches the same day. Some patients are able to home that day as well.
The worst of the pain typically eases within the first two weeks. You’ll start gentle physical therapy at home to rebuild strength and movement. Most people are back to enjoyable activities within a 6 weeks.
In term of getting back to work, most patient with desk jobs are able to get back to work in 3-4 weeks. Patients with job requiring manual labor, heavy lifting, navigating hazardous work sites, may require 3 months before they are able to return to work.
Physical therapy is ongoing. At three months the hope is that the hip is completely pain free, and you are functionally able to do all of you basic activities.
Full recovering may take a year, meaning it is not uncommon for there to be slight swelling, twinges of pain, or slight discomfort until you are fully healed.
After you heal, low-impact activities like walking, swimming, biking, hiking, and golf are all fine.
High-impact activities like running, jumping, or contact sports are not typically recommended, since they wear the new joint out faster. However, most patients who enjoy high impact activity are able to get back to it.
A successful hip replacement lasts 25 + years before it might need revision.
Major risks with this surgery:
Serious problems are uncommon, but no surgery is risk-free. The risk is a bit higher for people with long-term health conditions, who may also heal more slowly.
The main risks are:
- Infection: Bacterial can infect either at the skin wound or deeper in the tissue. Deep infections are rare but may need another surgery to clear completely.
- Blood clots: They form in the leg veins, which can be dangerous if they travel to the lungs. You’ll get blood-thinning medicine and exercises to lower this risk.
- Dislocation: Here, the new ball slips out of the socket, and needs to be manually placed back into the joint under sedation. It is most likely to happen early in recovery. Your surgeon will give you precautions to prevent it.
- Leg length differences: This is is less common now with advanced robotic surgery, but can occurs. Most of the time the difference is not noticeable.
- Loose implant: Over time a implant can become loose if it encounters high impact or the bone around the implant begins to break down.
There’s also one risk specific to the anterior approach: some people feel numbness on the outer thigh, because a nerve there can get pressed or stretched during surgery. Most patients have resolutions of this, but in some cases it can last long term.
What happens if you don’t have surgery:
Surgery is a choice, not a requirement. Many patients manage their hip for a long time without surgery. But it helps to know what to expect. Arthritis doesn’t heal on its own. It will tend to get worse as time goes on, because the damaged joint tends to keep wearing down over time.
For many people that means the pain slowly gets worse, the hip gets stiffer, and walking or everyday tasks become harder. Non-surgical treatments like medicine, injections, and physical therapy can ease symptoms and are worth trying. However, they manage the pain rather than fix the underlying problem.
The right time for surgery is different for everyone, and it’s a decision to make with your doctor based on how much your hip is affecting your life.
Do you have more questions?
Can anterior hip replacement surgery be performed on patients with hip dysplasia or deformity?
Anterior hip replacement surgery may be feasible for some patients with hip dysplasia or developmental abnormalities, but careful evaluation by an orthopedic surgeon experienced in complex hip reconstruction is necessary to determine the most appropriate surgical approach and implant selection.
Are there any specific recommendations for preventing falls or injuries during the recovery period?
Patients are advised to take precautions such as keeping walkways clear of obstacles, using assistive devices as needed, and following prescribed activity restrictions to minimize the risk of falls or injuries during the recovery period.
How is pain managed during the rehabilitation process after anterior hip replacement surgery?
Pain management during rehabilitation may include a combination of medications, physical therapy modalities such as ice therapy or transcutaneous electrical nerve stimulation (TENS), and gentle stretching and strengthening exercises to promote healing and mobility. During the course of your surgery and rehab, we provide non-opiate medication to allow you to engage in your rehabilitation effectively.
What types of assistive devices or aids are recommended during the recovery period after anterior hip replacement surgery?
Assistive devices such as walkers, crutches, or canes may be used initially to aid mobility and prevent falls during the early recovery phase. Gradual transition to walking aids and eventual independence is typically encouraged with ongoing rehabilitation.
Can patients with previous hip surgeries undergo anterior hip replacement surgery?
Yes, patients with previous hip surgeries may still be candidates for anterior hip replacement surgery. We have to factor in the nature of the previous surgeries, hip anatomy, and the patient’s overall health.
Are there any lifestyle modifications or adaptations needed for patients after anterior hip replacement surgery?
While most patients can resume their usual activities after anterior hip replacement, modifications such as avoiding high-impact sports and maintaining a healthy weight may be recommended to prolong implant longevity and maintain outcomes.
What factors might indicate the need for revision surgery following anterior hip replacement?
Factors such as persistent pain, implant loosening or wear, dislocations, or the position of implants may necessitate revision surgery. Regular follow-up appointments and monitoring of implant function are important for early detection of potential issues.
How soon after surgery can patients resume normal activities such as driving and household chores?
Most patients are back to driving around 4-6 weeks after surgery. Other household and functional activities are regained around this time as well. Everyone recovers at a different pace.
Can anterior hip replacement surgery be performed on patients with osteoporosis?
Yes, but careful consideration of bone quality and potential implant stability is necessary. Bone density assessments and consultation with a bone health specialist may be warranted in such cases.
Are there any restrictions on bending, twisting, or lifting following anterior hip replacement surgery?
Initially, patients are advised to avoid excessive bending or twisting of the hip joint and heavy lifting to prevent strain on the surgical site. Most of these restrictions are lifted around 3 months post surgery
What measures are taken to minimize postoperative pain and discomfort after anterior hip replacement surgery?
Various pain management techniques are used, including regional anesthesia (spinal or local), oral or IV pain medications, and non-pharmacological interventions such as ice therapy and positioning aids. Multi-modal pain management approaches are often used to reduced pain from every pathway and appraoch
How are patients monitored for complications during the recovery period after anterior hip replacement surgery?
Patients are closely monitored postoperatively for signs of complications such as infection, blood clots, or implant instability. Regular follow-up appointments and imaging studies may be conducted to assess healing and implant function.
Can anterior hip replacement surgery be performed on patients with severe hip deformities or abnormalities?
Anterior hip replacement surgery may be possible for some patients with severe hip deformities or abnormalities, but careful planning and assessment are necessary to ensure final outcomes.
What are the potential long-term effects or complications of anterior hip replacement surgery?
Long-term complications may include implant wear, loosening, or dislocation, which could necessitate revision surgery. However, with proper implant selection, surgical technique, and postoperative care, the risk of complications is low.
How long do patients typically stay in the hospital following anterior hip replacement surgery?
Hospital stays vary but are often shorter compared to traditional approaches, typically ranging from 1 to 3 days. Early mobilization and rehabilitation are key components of the recovery process.
Can anterior hip replacement surgery be performed on patients with metal allergies?
Yes, alternative implant materials may be available for patients with metal allergies, minimizing the risk of allergic reactions.
What type of anesthesia is typically used for anterior hip replacement surgery, and are there any alternatives?
Regional anesthesia (e.g., spinal or epidural) or general anesthesia are commonly used.
Are there any dietary supplements or vitamins recommended to support healing after anterior hip replacement surgery?
While not universally prescribed, supplements such as vitamin D and calcium may support bone health and aid in the healing process.
How soon after surgery can patients expect to see improvement in their hip pain and mobility?
Many patients experience immediate relief from hip pain following surgery. Improvement in mobility typically progresses over several weeks as swelling decreases and tissues heal.
What measures are taken to prevent infection during and after anterior hip replacement surgery?
Strict adherence to sterile surgical techniques, antibiotics before and after surgery, and meticulous wound care postoperatively are essential in minimizing the risk of infection.
Are there any specific exercises or activities to avoid after anterior hip replacement surgery?
Initially, patients should avoid high-impact activities and strenuous exercises that put excessive stress on the hip joint. Physical therapy will guide patients on appropriate exercises for rehabilitation.
Can anterior hip replacement surgery be performed on patients with hip fractures?
In certain cases, anterior hip replacement can be performed on patients with hip fractures, depending on the fracture type and patient’s overall health.
What are the potential risks or complications specific to anterior hip replacement surgery?
Potential risks include injury to nearby nerves and blood vessels, increased risk of fracture during surgery, and implant malpositioning. However, these risks are minimized with careful surgical technique and proper patient selection.
How does the recovery time for anterior hip replacement compare to traditional approaches?
Recovery time for anterior hip replacement is typically shorter compared to traditional approaches due to less disruption of muscles and soft tissues. Patients often experience faster mobilization and return to normal activities.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on June 8, 2026.

