Lumbar spine surgery is performed for patients experiencing severe pain, neurological symptoms, or instability due to various conditions, such as herniated discs, spondylolisthesis, and degenerative disc disease. The goal of the surgery is to relieve pressure on the nerve roots, stabilize the spine, and restore function. Procedures range from less invasive discectomy to more complex fusion surgeries, depending on the patient’s condition and needs.
How Common It Is and Who Gets It? (Epidemiology)
Spine issues, especially lumbar conditions like herniated discs and spondylolisthesis, are common, especially among individuals aged 30 and above. The risk increases with age, and certain factors such as obesity, smoking, and a sedentary lifestyle can exacerbate these conditions. Lumbar spine surgery is often considered when conservative treatments fail to alleviate the symptoms or when neurological functions are at risk.
Why It Happens – Causes (Etiology and Pathophysiology)
Conditions like herniated discs, degenerative disc disease, or spinal instability occur when the structures of the spine, such as discs or vertebrae, are damaged. These conditions can cause nerve compression, leading to pain, numbness, weakness, and sometimes paralysis. Over time, these degenerative conditions can lead to instability in the spine, making it necessary to perform surgical procedures like discectomy or fusion to prevent further damage.
How the Body Part Normally Works? (Relevant Anatomy)
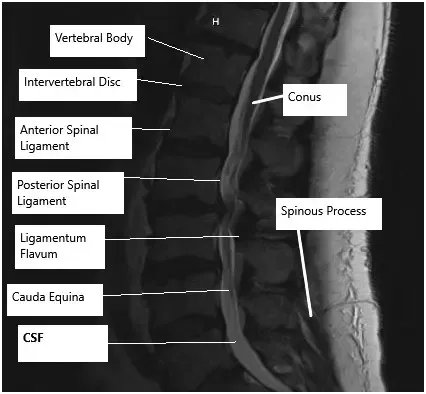
The lumbar spine consists of five vertebrae that support the lower back and allow for movement and flexibility. Between these vertebrae are intervertebral discs that act as cushions, absorbing shock. Nerve roots extend from the spinal cord through openings between the vertebrae. When discs bulge, herniate, or degrade, they can press on these nerves, causing pain, numbness, and weakness.
What You Might Feel – Symptoms (Clinical Presentation)
Symptoms of lumbar spine issues include persistent lower back pain, radiating pain down the legs (sciatica), numbness or tingling in the legs or feet, muscle weakness, and difficulty walking or standing for long periods. In some cases, the pain may worsen over time, limiting mobility and quality of life.
How Doctors Find the Problem? (Diagnosis and Imaging)
To diagnose lumbar spine issues, doctors use physical exams to assess mobility, reflexes, and strength. Imaging tests, such as X-rays, MRIs, and CT scans, help determine the extent of the damage, the location of nerve compression, and whether there is spinal instability. These images guide the decision-making process regarding the type of surgery required.
Classification
Lumbar spine surgeries are classified based on the condition being treated. For example:
- Discectomy is performed to remove part of a herniated disc.
- Laminectomy is done to remove part of the vertebra to relieve pressure on the spinal cord.
- Spine fusion is used to stabilize the spine when there is instability or deformity.
LUMBAR DISCECTOMY
This surgery is usually done for patients who have nerve root compression due to disc herniation, extrusion or sequestration. In this surgery, the aim is to remove the disc fragment, which is causing pressure on the nerve root. This surgery is done for the back and a limited amount of bone is removed as far as we get access to the disc. The disc fragment, which is causing pressure on the nerve root is removed and the nerve root is checked to be free of any pressure. This surgery does not involve removal of enough bone to need stabilization surgery or fusion surgery. The patients after the surgery usually recover well within the next 3 to 6 weeks.
DECOMPRESSION OR FORAMINOTOMY
This surgery is usually done for the patients who have nerve root compression at the level of the foramina. This surgery is done from the back and usually involves removal of a small amount of bone, which is not enough to cause instability. This surgery is not associated with fusion surgery. The patients recover well after the surgery in over the next 4 to 8 weeks.
LAMINECTOMY
Laminectomy involves removal of the bone from the back of the nerve roots. This was performed at one or multiple levels depending on the level of stenosis. This surgery is done from the back. This surgery allows decompression of the nerve roots within the spinal canal. It is consistent and good results and the patients recover well over the span of 6 to 12 weeks.
SPINE FUSION
Spine fusion in the lumbar area is usually performed for instability of the spine or spondylolisthesis. This involves fixation of the vertebrae with screws and rods. It can be done at multiple levels depending on the need. This surgery is usually associated with cleaning of disc space and replacing it with cage and bone graft to make the adjacent vertebrae fuse. This surgery is most commonly performed from the back though it can be performed from the front as well as from the side too. The patients who undergo this surgery usually must be admitted in the hospital for 3 to 5 days and the recovery is gradual for a period of 8 to 12 weeks.



Castle nut driver used in minimally invasive posterior spinal fusion
The images above show the instruments used in minimally invasive posterior spinal fusion. The minimally invasive technique utilizes the percutaneous incisions to minimize soft tissue trauma. The technique may result in early rehabilitation and reduced post-operative pain.
Other Problems That Can Feel Similar (Differential Diagnosis)
Other conditions, such as muscle strain, sciatica, or conditions affecting the hip or pelvis, can cause symptoms similar to lumbar spine problems. These conditions need to be ruled out to confirm a diagnosis of lumbar spine pathology.
Treatment Options
Non-Surgical Care
- Medications (e.g., NSAIDs, pain relievers) to manage pain and inflammation.
- Physical therapy to strengthen muscles and improve mobility.
- Bracing to support the spine and reduce strain.
- Injections (e.g., corticosteroids) to reduce inflammation and pain.
Surgical Care
- Discectomy: Removal of part of a herniated disc to relieve nerve pressure.
- Laminectomy: Removal of bone from the spine to relieve pressure on the spinal cord.
- Spine Fusion: Fusing two or more vertebrae together to provide stability, often using screws, rods, and bone grafts.
Recovery and What to Expect After Treatment
Recovery varies depending on the procedure:
- Discectomy: Most patients experience significant pain relief within a few weeks. Physical therapy is usually recommended.
- Laminectomy: Recovery typically takes 6 to 12 weeks. Patients may need to restrict activities to ensure proper healing.
- Spine Fusion: Recovery is more prolonged, usually taking 8 to 12 weeks. Patients may require a brace and physical therapy.
Possible Risks or Side Effects (Complications)
As for all surgeries there are certain but rare risks for anesthesia including cardiac arrest, stroke, paralysis, and rarely death.
Risks of Lumbar spine surgery may include though not limited to:
- Hematoma or hemorrhage
- Damage to the major vessels which may result in excessive bleeding, even death
- Blindness
- Damage to the dura, resulting in a cerebrospinal fluid leak
- Failure, loosening or pull out of the cage, graft, rod or screws
- Wound infection
- Failure of fusion to happen
- Damage to the nerve root(s) resulting in new onset or deterioration of preexisting pain, weakness, paralysis, loss of sensation, loss of bowel or bladder function, impaired sexual function, etc., which may or may not recover.
- A few of these conditions may warrant repeat surgery
Certain patient population is at a higher risk for complication which include but are not limited to:
- Smoking
- Seizures
- Obstructive sleep apnea
- Obesity
- High blood pressure
- Diabetes
- Other medical conditions involving your heart, lungs or kidneys
- Medications, such as aspirin, that can increase bleeding
- History of heavy alcohol use
- Drug allergies
- History of adverse reactions to anesthesia
Long-Term Outlook (Prognosis)
For most patients, lumbar spine surgery provides significant relief from pain and improved mobility. The long-term outlook depends on the type of surgery and the severity of the condition. Fusion surgeries may provide lasting stabilization, while some patients may require further treatments or adjustments.
Insurance & Cost
Lumbar Spine Surgery at Complete Orthopedics is covered by Medicare and most major insurance carriers (Aetna, Anthem BCBS, Cigna, Empire BCBS, UnitedHealthcare), as well as most workers’ compensation and no-fault insurance plans. Your out-of-pocket cost depends on your specific plan, deductible, and the medical necessity criteria that apply to your case.
Call our billing team at (631) 981-2663 before scheduling to verify your coverage and discuss expected out-of-pocket costs. For the full list of carriers we accept and patient billing protections, see our Insurance Information page.
Frequently Asked Questions (FAQ)
Q. How long does it take to recover from lumbar spine surgery?
A. Recovery varies by procedure. Most patients recover from a discectomy within a few weeks, while full recovery from a spine fusion may take 8 to 12 weeks.
Q. Is lumbar spine surgery safe?
A. While lumbar spine surgeries are generally safe, they carry risks such as infection, nerve damage, and complications from anesthesia. Careful selection of patients and proper technique minimize these risks.
Q. Will I need physical therapy after surgery?
A. Yes, physical therapy is typically recommended to restore strength and flexibility after lumbar spine surgery.
Summary and Takeaway
Lumbar spine surgery, including discectomy, laminectomy, and spine fusion, offers effective treatment for conditions such as herniated discs, spinal instability, and nerve compression. While the recovery time and potential risks vary depending on the procedure, most patients experience significant pain relief and improved function. It is important to work closely with a spine specialist to determine the best treatment plan for your condition.
Clinical Insight & Recent Findings
A recent study by Haddas et al. (2025) provides a comprehensive review of postoperative exercise and rehabilitation following lumbar spine surgery, with a particular focus on its impact on outcomes such as pain, function, and mobility. The review suggests that supervised therapeutic exercise is beneficial and safe for patients recovering from lumbar discectomy, fusion, and total disc replacement surgeries.
Early initiation of therapeutic exercises, tailored to individual patient needs and surgical factors, can improve long-term recovery, reduce opioid dependency, and enhance physical function. The study highlights that exercise protocols should consider patient-specific variables such as prior function, comorbidities, and tissue healing timelines, and it emphasizes the importance of progression from basic to more complex movements as part of a graded recovery plan.
Wearable technology and physical activity monitoring are also emerging as valuable tools in enhancing postoperative rehabilitation, enabling continuous tracking of patient activity and progress. (“Study of postoperative rehabilitation following lumbar spine surgery – See PubMed.”)
Who Performs This Treatment? (Specialists and Team Involved)
Lumbar spine surgery is typically performed by orthopedic spine surgeons or neurosurgeons who specialize in spinal conditions. The surgical team may also include anesthesiologists, surgical assistants, and nurses.
When to See a Specialist?
- temperature more than 101 degrees Fahrenheit
- increased pain or tenderness near the incision
- poor pain relief
- signs of infection: increased swelling, redness, increased drainage, increased warmth, pus, foul smell, bleeding at the incision, incision coming apart
- increased numbness, numbness in genital area
- inability to feel or move fingers or toes
- pale blue, white or abnormally cold fingers or toes
- nausea (upset stomach) or vomiting (throwing up) that won’t stop
- increased tiredness
- a generally worse feeling than you had when you left the hospital
- problems urinating, severe constipation or severe diarrhea
- a concern about any other symptoms that seem unusual
When to Go to the Emergency Room?
- Suspected cardiac problem: severe chest pain or pressure, shortness of breath, tightness in chest, pain in left arm, jaw pain, dizziness or fainting, unexplained weakness or fatigue, rapid or irregular pulse, sweating, cool, clammy skin, and/or paleness
- Suspected Stroke: trouble speaking, changes in vision, confusion or other change in mental status
- Suspected venous thrombosis: swelling of the legs, ankles, or feet, discomfort, heaviness, pain, aching, throbbing, itching, or warmth in the legs, sudden shortness of breath, chest pain, coughing up blood, rapid or irregular heart rate
- Suspected Sepsis: high grade fever, with shivers associated with fatigue, dizziness, racing heart, pale or discolored skin, sleepy, difficult to rouse, confused, short of breath
- Heavy bleeding from the surgical site
- Severe allergic reaction with trouble breathing, swelling, hives
What Recovery Really Looks Like?
After lumbar spine surgery, most patients experience significant pain relief. Recovery times vary, but most can return to light activities within a few weeks, with full recovery taking 8 to 12 weeks.
What Happens If You Ignore It?
If left untreated, conditions like herniated discs or spinal instability can lead to chronic pain, permanent nerve damage, or even paralysis. Surgery can alleviate symptoms and restore function.
How to Prevent It?
Maintaining good posture, regular exercise, and a healthy weight can help prevent spine problems. Strengthening core muscles and practicing proper lifting techniques can reduce the risk of injury.
Nutrition and Bone or Joint Health
A balanced diet rich in calcium and vitamin D supports bone health. Regular weight-bearing exercises and hydration are also important for maintaining a healthy spine.
Activity and Lifestyle Modifications
Post-surgery, avoid heavy lifting and intense physical activities in the early recovery stages. Gradual, low-impact exercises can help strengthen the spine and maintain flexibility.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on July 2, 2026.
