Patient is a 16 year-old male with complaints of wrist pain after he was riding his quad prior to arrival and accidentally fell off landing on his right wrist. Patient denies any other injuries.
Patient went to urgent care and was told his right wrist may be fractured; however, no imaging was done. Patient was put in a right arm sling. Patient denies any numbness, tingling, fever, or any additional complaints.
Patient advised to undergo X-ray to assess his wrist condition. Found significant results, there are fractures of the distal right radius and ulna styloid. CT scan also requested, confirmed the comminuted distal radial and ulnar styloid fractures.

MRI of the wrist
We discussed treatment options and opted for surgical management. We discussed risks of Infection, bleeding, injury to adjacent nerves and vessels, among others. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. The right upper extremity was prepped and draped aseptically in the usual fashion. Tourniquet was applied. Preoperative antibiotics were given. Time-out was called. Tourniquet was elevated to 250 mmHg. Tourniquet time was 61 minutes.
Provisional fixation of the fracture was done after reduction using a volar incision was driven along the tendon of the flexor carpi radialis. The anterior sheath of flexor carpi radialis was opened. The tendon was retracted medially.
The posterior sheath for the tendon was opened and the pronator quadratus was reached. The pronator quadratus was incised along the radial border. Fracture was opened. The fracture was thoroughly washed. Reduction of the fracture was again done and the wires were re-inserted.
A short plate was applied under the volar aspect of the radius and fixed with olive wires. X-rays were done to check the satisfactory position. The fixation of the plate to the proximal fragment was done by a single unicortical screw.
‘Finding the fracture and the plate in acceptable position, the distal fragment was fixed using locking screws Including two radial styloid screws. The first screw was a cortical screw to pull the plate to the bone. The cortical screw was wasted at the end of the procedure.
The proximal fragment was fixed using a combination of locking and nonlocking screws. Final fixation of the plate was checked in AP and lateral views and found to be satisfactory.
Transfixation of the radioulnar joint was performed using K-wires. The final pictures were taken in AP and lateral views and saved. The wound was thoroughly washed and closed In layers using # 2-0 Vicryl and # 4-0 Monocryl.
Dermabond was used for the skin. Dressing was performed using 4 x 4s, Xeroform, Webril, posterior long arm splint, and Ace wrap. The patient was moved to Recovery in a stable condition.
After one-week post-operative the patient was advised to return with X Ray results. Result was presented and discussed the surgically treated fracture of the right wrist. He is doing well and will continue the long arm splint.
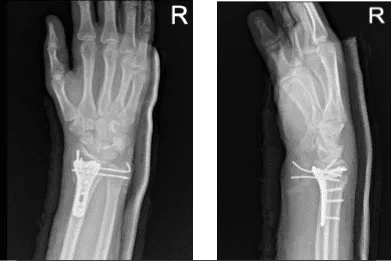
Right wrist X-ray 3 or more views-1st week post operative
Two weeks post operative passed. Xray reviewed and showed fracture fragments appear in good position and alignment.
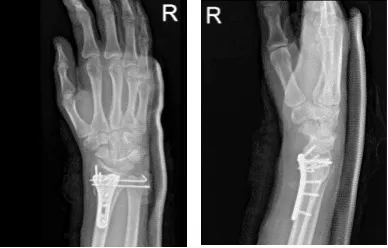
Right wrist X-ray 3 or more views-2nd week post operative
4th week post operative, considering the wires were poking under skin and imminent to break it, we decided to remove the wires and long arm splint to continue. Xray result reviewed.

Right wrist X-ray 3 or more views-4th week post operative
At 32 weeks post operative, the patient tolerated activities and returned to his normal routine. Patient gets well from his surgery with consistent visits to our office.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
