Quadriceps tendon repair for the ACL, or anterior cruciate ligament an autograft is a surgical treatment where a portion of the quadriceps tendon extracted from your own leg is used to repair or reconstruct a ruptured ACL ligament in your knee. Located above the patella or kneecap, the quadriceps tendon is a thick tissue.
A ripping or popping feeling is frequently felt when a patellar tendon ruptures. Usually, you’ll have pain and swelling, and you could be unable to straighten your knee. The patellar tendon tore, leaving an indentation at the base of your kneecap as additional symptoms.
A 26 year-old patient was in our office with complaints of left knee pain. He was in with x-rays of his left knee. For aggravating factors, patients reported standing, walking, lifting, twisting, pushing/pulling, throwing, rom, weight bearing, exercise, previous surgery, upstairs, downstairs, and nighttime.
For associated symptoms, he reported weakness, numbness, tingling, swelling, redness, warmth, popping/clicking, buckling, instability, radiation, tender to the touch, and pain with motion but reports no redness, no ecchymosis, no grinding, no radiation, no fever, no chills, no weight loss, and no change in bowel/bladder habits.
For location, left. For quality, he reported aching, burning, stabbing, throbbing, sharp, frequent, constant, and no change. He is currently employed as an electrician. He is not able to bend or extend the knee and is hopping with a limp and not able to bear weight on the foot.
The patient presented X-ray results which showed that there is mild lateral compartment joint space narrowing. Otherwise unremarkable. Positioning is suboptimal as the patient is unable to straighten his knee.
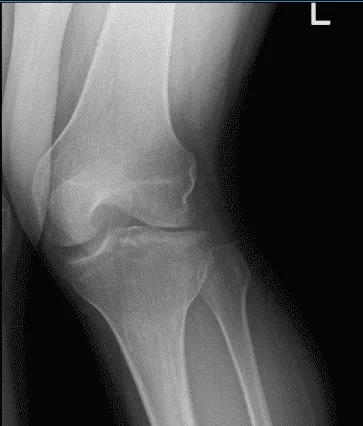
Left knee X-ray AP and Lateral with Oblique 3 views
For his MRI, the result showed abnormal morphology of the ACL likely related to partial disruption or possibly complete disruption (images limited by motion). Medial meniscus bucket-handle tear.
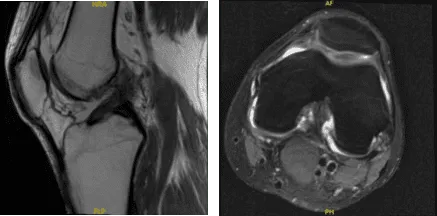
MRI-3T Left knee non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, need for rehabilitation, possibility of failure, need for repeat surgery, development of knee arthritis and possible need for knee replacement in the future, among others.
We also discussed systemic complications including blood clot, cardiac, neurologic, or pulmonary complications among others. The patient understood and signed an informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was induced. His left lower extremity was prepped and draped aseptically in the usual fashion after application of tourniquet. Preop antibiotic was given.
Examination under anesthesia was performed which showed ACL laxity or Lachman test with no end point. A lateral entry portal was made. Arthroscope was entered and a medial entry portal was made with the help of spinal needle.
Examination of the knee showed a bucket handle medial meniscus tear right from the posterior horn to the mid body. It also showed avulsion and injury to the ACL with collapse. The lateral compartment showed no tear or injury. Patellofemoral compartment was normal. We decided to harvest the quadriceps autograft as was planned.
The arthroscope was removed and a 3-cm incision was given over the proximal pole of the patella. The subcutaneous tissue and paratenon were cut in the line of excision. RayTec was used to delineate the tendon. Arthrex preset quadriceps harvest double knife was used and the tendon was cut on either side.
The distal end was elevated from the proximal pole of the patella using a blade. Proximally, the tendon was cut through the intrasubstance. Tendon cutter was used to harvest 18 mm of tendon. FiberTape was applied over the proximal femoral side. Tendon was prepared on the back table and the tibial side was also prepared.
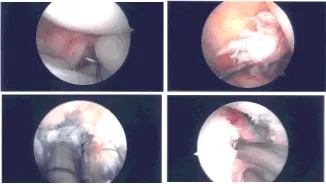
Intraoperative Arthroscopy Images
In the meantime, an arthroscope was inserted into the knee again. Inside out repair of the medial meniscus was planned using zone-specific cannulas from the meniscus were used. Sequential from the posterior horn to the mid body. All the needles were retrieved out of the medial knee.
The needles were cut and the sutures were held by a hemostat. ACL debridement was performed. The femoral attachment of the ACL was prepared using the shaver. Tibial attachment was also prepped using the shaver.
ACL femoral jig was used and inserted. Incision was given over the lateral femoral condyle and the fascia was cut in the line of Incision. The Jig was introduced into the knee and connected The jig was passed onto the bone and punched inside.
FlipCutter was used and drilled into the knee. Once the drill was inside the knee, it was flipped back and a 25-mm turnover was made. The reamer was again inserted back into the knee and flipped back to the normal position and retrieved out. A FiberLink was inserted and retrieved.
Similarly, a tibial tunnel was made using a tibial jig for the medial portal. A 60-degree angle was used. FlipCutter was used again to make a 30-mm tunnel in a similar fashion. A FiberLink was inserted and the suture was held on to each other.
Once the quadriceps tendon was ready, it was marked and inserted over the FiberLink on the femoral side and passed into the tunnel. Then, the tibial side was also passed to the tibial tunnel using the FiberLink.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
