Human shoulder is known as the most extensive range of motion in the human body. Our muscles in our shoulders help us to abduct, adduct, flex, extent and rotate.
Based on research, there are three common injuries on the human shoulder: instability, frozen shoulder and the popular rotator cuff tear. In this article, rotator cuff tears will be tackled. Without treatment, rotator cuff tear may lead to permanent loss of motion.
Patient is a 32 year-old male and has complaints with his left shoulder, neck and back pain after getting involved in a motor vehicle accident. Per patient, neck and back pain is tolerable but his shoulder is in extreme pain. We decided to get Xray for us to see the reason behind it. X Ray impression showed Acromioclavicular joint arthropathy.

MRI of the shoulder
We did an MRI which showed a paralabral cyst and this labral tear extending into the posterior superior labrum. We discussed treatment options and opted for surgical management.
We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, need for repeat surgery, need for rehabilitation, restriction of movement and need for extensive physical therapy, systemic complications including blood clots, cardiac, pulmonary, neurological complications, and death. The patient understood and signed an informed consent.
The patient was taken to the operating room, where supraclavicular necks were given and general anesthesia was induced. Preoperative antibiotics in the form of 3 g of Ancef was given.
The patient was put in a right-side position with left shoulder up. Left shoulder was put on antibiotics and draped aseptically in the usual fashion and put on traction and 45 decreased abduction and flexion. A posterior entry portal was made. Arthroscope was entered.
There was labral tearing along the anterior superior part along with tenting of the superior labrum and the biceps. An inferior portal was made with the use of a spinal needle. Shaver was introduced due to some debridement of the labrum of the biceps. Examination showed type 2 SLAP tears.
Anterosuperior portal was made along without a spinal needle. Shaver was introduced to prepare for labral tears. Rasp was introduced from the anterosuperior portal and glenoid as well as labrum was swept along the superior and then the pledged on the posterosuperior labrum.
Posterosuperior portal was also prepped. The labrum. A 25 degree to the right suture crossing chain that was used from Arthrex. Three sutures were passed from the superior to the posterior labrum. Two PushLock were used to pass the 1.3 mm of the margins.
The fixation of labral tapes and to place these labral tapes into the labrum was found to be adequate. Picture was taken. The shoulder was debrided. Shoulder was swollen in the process and it was decided not to do a subacromial examination at the moment considering the symptoms from the labrum.
The biceps was already cut from the labrum for preparation for mini open biceps tenodesis. The scope was removed and subpectoral skin incision was given along the inferior margin of the pectoralis major.
Deltopectoral fascia was cut. The pectoralis major was retracted laterally and bone was reached. The bicipital groove was reached and the tendon was retrieved with the use of right angle forceps. The bed for the biceps was prepped with the use of Bovie followed by bicortical and a unicortical screw drill.
The tendon was prepped with the use of FiberWire. EndoButton was used to pass bicortically and flipped. The tendon was further fixed using the #7-0 EndoButton. The sutures were tied off with the tendon itself twice in the process.
Final pictures of the Incision was thoroughly washed and drained. Closure was done in layers using #0 Vicryl, # 2-0 Vicryl and Monocryl. Dressing was done with use of 4 x 4s followed by ABD, tape. Shoulder immobilizer was applied. The patient was extubated and moved to recovery in a stable condition.
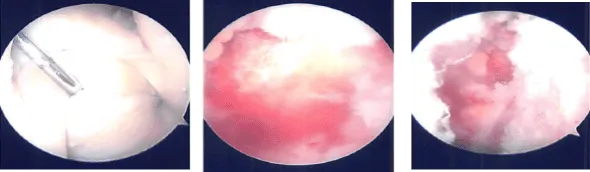
Intraoperative images
After a week post-operative, a patient came into the office to discuss the treatment options. We have decided to proceed with formal physical therapy as well as a home exercise program for the rehabilitation of her shoulder.
Stitches were removed. Patient will continue the ice and elevation for it helps with her condition. Patients regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
