The knee is one of the largest joints in the human body. It enables us to do simple actions such as standing, walking, running, and maintaining human equilibrium. Knees have cartilage, such as meniscus, and ligaments, such as the LCL, MCL, ACL, and PCL.
A medial meniscus tear is a common knee condition among athletes, but anyone of any age can tear the cartilage with fast twisting movements of the knee. This condition can progress to more serious injuries, such as arthritis; the medial meniscus is more commonly affected than the lateral meniscus, resulting in pain, stiffness, swelling, locking, and other symptoms.
A 27-year-old male patient was seen in the office, with complaints of pain in the right knee for about five days. The patient remembers his injury in a motor vehicle accident.
The pain is severe to extreme in intensity associated with sharp, dull, stabbing, throbbing, aching, burning with swelling, bruising, weakness, gait problem, giving way and limping. The problem has been getting worse since it was started. The usual routine of the patient like walking, standing, lifting, exercise, twisting, bending, stairs, make the symptoms worse.
MRI results were presented and reviewed by the doctor. It showed that there is medial meniscus tear right knee on the periphery sort of also ramp lesion. We discussed treatment options and the patient opted for surgical management.
We discussed risks, benefits, and complications of surgical management including bleeding, infection, injury, adjacent nerve and vessels, heed for repeat surgery, rehabilitation, need for wearing a knee immobilizer, and among others. The patient understood and signed an informed consent.
The patient was taken to the operating room, where he was placed on a well-padded operating room table. General anesthesia was induced. A tourniquet was applied on the mid-thigh of the right side. After the preoperative antibiotics were given, the right lower extremity was prepped and draped in an aseptic condition and the tourniquet was inflated.
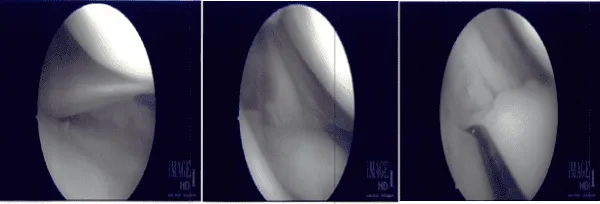
The lateral entry portal was made and the arthroscope was introduced. The Patellofemoral joint and the medial compartment was examined and there was near complete tear of the posterior horn of the medial meniscus from the capsule. The decision to repair it was taken.
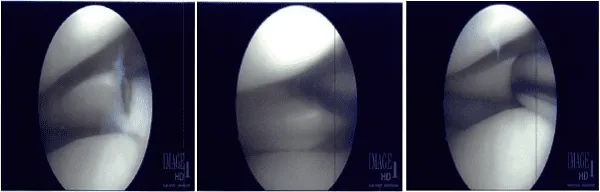
The margins were probed using rasp and shaver. The meniscus was approximated onto the capsule and fixed using FasT-Fix Nephew curved x2. Good opposition was achieved. The sutures were cut after the notch. All-inside technique was used. Lastly, in the intercondylar area the scope was moved, the ACL was found to be intact.
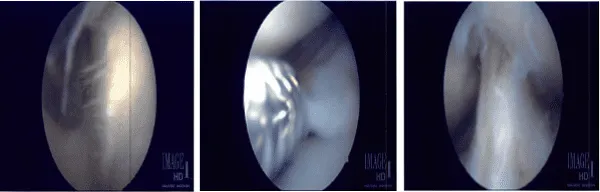
The scope was moved to the lateral compartment, where there was faying of the posterior horn near the root of the lateral meniscus. It was debrided using shavers and punch. The scope was moved to the patellofemoral joint, which was found to be in good condition.
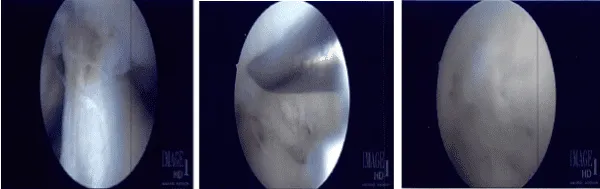
The lateral meniscal tear was further debrided and the final pictures were taken. At the end of the procedure, micro punch was also used to put 4 to 5 holes into the intercondylar area.
Fat globules and fresh blood could be seen coming out of hose holes. The knee was irrigated copiously and closed using nylon #4-0. Dressing was done with Adaptec, 4×4, Web il, and Ace wrap.
After a week of seeing patients, he has been improving with regards to pain and swelling. He is limping and has been using crutches for ambulation. Denies fever, chills, reinjury. After two weeks post-surgery the incisions are healed. Tenderness over the medial side of the knee from the condyle to the pes.
Also tender anterior ally, over the tissues inferomedial to the patella. No patellar apprehension sign Stability to medial lateral stress revealed soft end point on right at a similar point as the right knee. No rotatory instability or asymmetry side to side. 30-degree flexion is the most comfortable position.
Range of motion 20-50. Positive straight leg raises. Strength distally is 5/5. There is no calf tenderness and a negative Homan’s sign. Decreased sensation over the lateral side of the right knee. Sensation is intact to light touch distally and there is a brisk capillary refill. There is a full range of motion without discomfort.
However, we advised the patient to wear a Bledsoe brace and ambulate with it fixed in full extension only and do formal physical therapy as well as a home exercise program for rehabilitation of the knee.
Patients regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
