Patient is here with complaints of right knee pain. He is 57 years of age. He stated that he accidentally twisted his knee while walking. He currently works as a FedEx mechanic whose work describe as he inspects vehicle components that may require him to bend or lift his knee.
X-ray reviewed and discussed and suspected to have a tear meniscus. We agreed to have an MRI to see the reason behind it. His MRI Impression as follows: There is an acute tear of the mid anterior cruciate ligament with contusions in the lateral femoral condyle and posterior lateral tibial plateau.
There is a nondisplaced subcortical fracture of the posterior lateral tibial plateau. There is also contusion in the medial femoral condyle. Radial tear of the posterior horn of the medial meniscus at the level of the meniscal root attachment with extrusion of the body.
Lateral subluxation of patella with moderate chondromalacia in the apex. Large joint effusion with synovitis. There is a strain of the popliteus muscle.
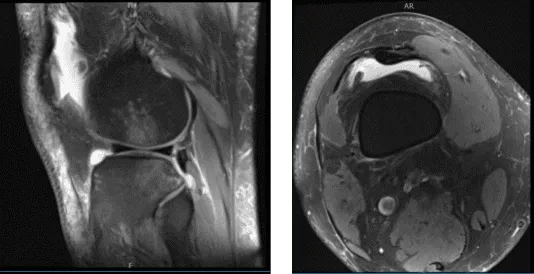
MRI of knee
FlipCutter was used and drilled into the knee. Once the drill was inside the knee, it was flipped back and a 25-mm turnover was made. The reamer was again inserted back into the knee and flipped back to the normal position and retrieved out.
A FiberLink was inserted and retrieved. Similarly, a tibial tunnel was made using a tibial jig for the medial portal. A 60-degree angle was used. FlipCutter was used again to make a 30-mm tunnel in a similar fashion. A FiberLink was inserted and the suture was held on to each other.
Once the quadriceps tendon was ready, it was marked and inserted over the FiberLink on the femoral side and passed into the tunnel. Then, the tibial side was also passed to the tibial tunnel using the FiberLink.
Once the tendon was in place, it was tightened on either side and found to be in a good position. The graft was tightened over the tibial side and was tightened over the button along with two 4.7 size SwiveLock. The knee was cycled 30 times before final tightening.
The knee was thoroughly irrigated. The final pictures were taken and saved. The tendon was found to be in good tension. Notchplasty of the lateral femoral condyle was performed also. The final pictures were taken and saved. Tourniquet was released at this time.
Now, posteromedial incision was given along the posterior margin of the MCL. Blunt dissection of the subcutaneous tissue and fascia was done. All the sutures were retrieved along the posterior margin of the capsule and the lateral margin of the capsule. All the sutures were tied on each other and cut.
The incision was thoroughly irrigated and closed in layers using # 2-0 Vicryl and Monocryl. The quadriceps harvest incision was also closed with # 2-0 Vicryl and Monocryl.
The arthroscopic portal as well as tibial and femoral ACL groove tunnel were closed using #3-0 nylon. Dressing was done using 4 x 4, ABD, Webril, and Ace wrap. A knee immobilizer was applied after the surgery. The patient was extubated and m
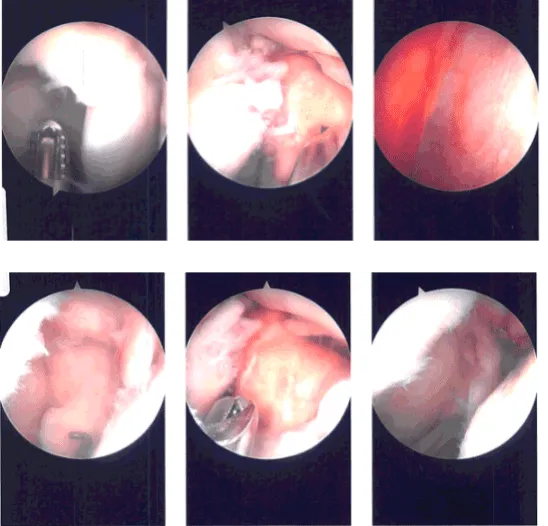
Intraoperative Arthroscopy Images
After discussing the options for treatment and the risks of aspiration and injection, the patient wished to proceed with the aspiration and injection to reduce pain and swelling. After a sterile prep, and the injection of a local anesthetic, 90 cc of straw-colored fluid was aspirated from the left knee joint.
This was followed by an intra articular injection, consisting of 60 mg or Toradol followed by 1 cc of 1% lidocaine, 1cc of 0.5% Marcaine. The patient tolerated the procedure well and there were no complications.
Post aspiration pain, and the signs of infection were discussed in detail. Patient checked in for a follow up visit after a month and saw significant improvement on his knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
