Open reduction and internal fixation, often known as ORIF, is a surgical procedure used to repair fractures in order to enhance function and range of motion. The largest of the two forearm bones is the radius.
The distal radius is the portion of the radius that connects to the wrist joint. The most common cause of a radius fracture at the wrist is falling on an extended or flexed hand.
The patient is a 49 year-old male, seen in the office with injury to the left wrist following a fall. A closed reduction was tried in the hospital which failed. We discussed treatment options and opted for surgical management.
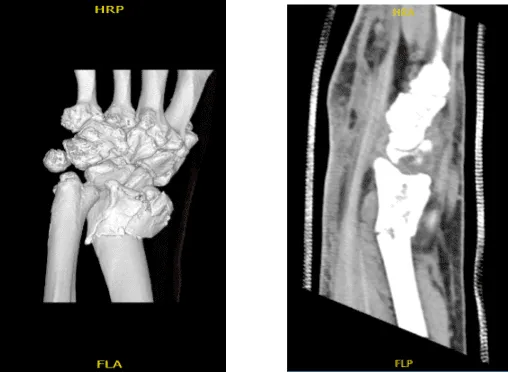
An MRI was reviewed and discussed by the doctor; a comminuted distal radial fracture is present with intra-articular extension where displacement measures up to 3 mm. Ulnar angulation is also present. Degenerative changes are present at triscaphe and first carpometacarpal joints.
Soft tissue edema is present around the wrist. We also discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, nonhealing, nonunion, need for repeat surgery, arthritis, need for rehabilitation, systemic complications including blood clot, cardiac, all pulmonary and neurovascular complications including death.
Considering the risks and benefits, the patient signed the informed consent.
Left wrist pain
The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. Left upper extremity was prepped and draped aseptically in a usual fashion.
A tourniquet was applied. Tourniquet was inflated and the tourniquet time of 63 minutes was used at 250 mmHg. Volar incision was driven in line with the flexor carpi radialis tendon. The anterior sheath of the flexor carpi radialis tendon was cut in the line of incision.
The tendon was retracted medially and the posterior tendon was cut. Pronator quadratus was reached, which was cut along the radial border. The fracture site was opened and irrigated.
The fracture was comminuted in more than three parts with intraarticular extension. The fracture was reduced manually and then fixed with multiple K-wires and checked under fluoroscopy. Finding it in an acceptable position, a volar plate was put and fixed with the use of ball-tipped K-wires.
The picture was then again taken to confirm the good reduction. The plate was fixed to the fracture with the use of locking and nonlocking screws. One Screw was wasted. to pull the distal fragment with the plate also. Pictures were taken in between and then the final picture was taken and saved. They were found to be in an acceptable position.
The wound was then thoroughly irrigated. Tourniquet was released and hemostasis was achieved. Surgery was put in to achieve further hemostasis. Closure was done in layers using #2-0 Vicryl and #3-0 Monocryl for subcu and subcuticular closures.
Dressing was done with the use of Xeroform, ABD, 4 x 8s, and Webril. Short arm splint and Ace wrap was applied. The patient was extubated and moved to recovery in stable condition.
After two weeks the patient was seen in the office for his post operative visits, with x-rays of his left wrist. It showed that the surgical plate and screws traverse an incompletely healed oblique fracture of the distal left radius. Hardware appears intact.
There are mild degenerative changes of the first carpometacarpal joint. There are no subluxations nor dislocations and there are no radiopaque foreign bodies and mild soft tissue swelling is noted. Aside from that, the patient denies fever, chills and the pain are well controlled.
We agreed to go with conservative management for now and PT to be started and discussed also the splint was to be discarded and brace to be applied.
After the operation, the patient recovered well and kept up with physical therapy. After a month, the patient returned for a follow-up visit and his wrist had much improved.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy
