Patient is in our office, with complaints of bilateral knee pain but she complaint that left main is the most painful. The pain started over a week ago. The patient remembers an injury in a fall, where her right foot got caught in concrete and tripped.
Patient had gone to ER afterwards. The pain is associated with swelling, bruising, numbness, tingling, and radiating pain. The pain is getting worse from the day it started. Ice and tramadol help but temporarily only.
Upon examination of the right and left knee, the patient is tender to palpation along the medial tibial condyle and joint line. The patient has discomfort with McMurray’s maneuvers, and the knee is stable.
They lack full flexion secondary to the effusion, but have full extension. They have 5/5 strength, and are neurovascularly intact distally. There is no erythema, warmth or skin lesions present.
X-ray results presented and reviewed showed that there are no degenerative diseases. Advised patient to undergo MRI and found out that there is subcutaneous edema anteriorly and anteromedially.
Suspected tear in the posterior horn of the medial meniscus. There is a very faint oblique signal that appears to extend to the inferior articular surface. There is partial tear of the proximal PCL and mild chondromalacia patella and deep infrapatellar bursitis were also observed.
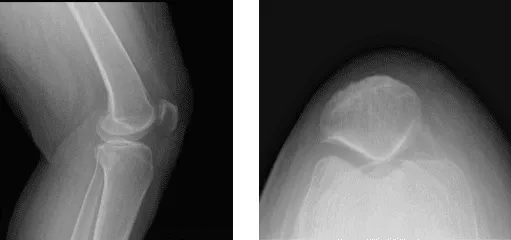
Left Knee X-ray Complete with patella
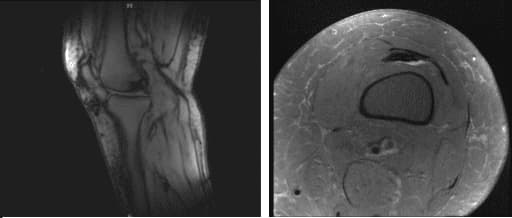
MRI-3T Left Knee Non-contrast
We discussed treatment options and opted for treatment of the right knee as well as pes anserine bursitis, trochanteric bursitis of the right side. She has also planned for having a left shoulder surgery in the future.
We discussed treatment options and planned to do arthroscopic examination and surgery of the left knee as well as cortisone injection of the right lower extremity.
We discussed risks, complications, and benefits including infection, bleeding, injury to adjacent nerves and vessels, recurrence of tears, need for repeat surgery, need for cortisones in the future, need for rehabilitation, systemic problems like blood clot, neurological,pulmonary, cardiac problems among others. The patient agreed and signed an informed consent.
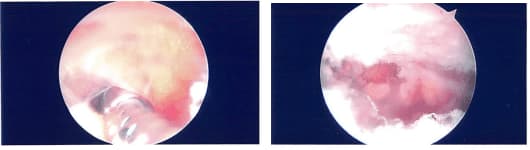
The patient was taken to the operating room where she was placed on a well-padded operating room table. Left lower extremity was prepped and draped aseptically. A time-out was called. Preoperative antibiotics were given. Tourniquet was Inflated.
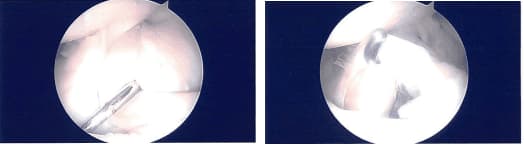
Lateral entry portal was made and the scope entered. There was ____ In the patella as well as on the medial femoral condyle which after making a medial portal, cleaned arthroscopically using a shaver.
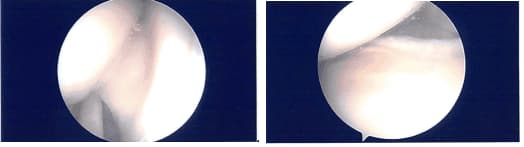
Examination of the medial meniscus showed a tear of the anterior horn of the medial meniscus which was clean. The intercondylar notch showed an intact ACL. Lateral tibiofemoral compartment examination was normal.
After thorough Irrigation, final pictures were saved and the wound was closed. Then, 40 mg of Depo-Medrol was injected in the left knee after the surgery.
Prior to the start of the left knee surgery, 40 mg of Depo-Medrol mixed with 3 cc of ropivacaine was injected each in the right pes anserine bursa, right knee joint as well as right trochanter. Dressing of the left knee was performed and the patient was extubated and moved to the preop in stable condition.
After a week of seeing patients, he has been improving with regards to pain and swelling. He is limping and has been using crutches for ambulation. Denies fever, chills, reinjury. After two weeks post-surgery the incisions are healing well, without evidence of drainage, erythema or warmth.
There is a full range of motion without discomfort. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee.
The patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
