Knee arthroscopy is a procedure that employs a tiny camera to examine the interior of your knee. Arthroscopic meniscectomy is a minimally invasive outpatient surgical treatment used to repair a torn meniscus cartilage in the knee.
A 51 year-old patient female who was seen in the office with complaints of pain on the right knee. She presents with right knee and left hip pain which began a month ago.
She has been having pain in the knee for several months but it started buckling, giving way and swelling since last 4 weeks. She has been trying exercises by herself but has had worsening of the knee. She tried conservative management, which did not help.
We agreed to go with 3 tesla MRI of Right knee, the results were reviewed and discussed by the doctor, there is no acute fracture or osteonecrosis. The Ligaments, cruciate and collateral ligaments are intact, the Lateral compartment meniscus demonstrates a partially discoid configuration.
There is a partial superior articular surface tear within the anterior horn of the lateral meniscus (sagittal image 14). No full-thickness cartilage defect is seen, there is tiny marginal osteophytosis.
Medial compartment is intrasubstance degenerative signal within the body and posterior horn of the medial meniscus without extension to an articular surface to constitute tear.
Mild free edge margin fraying is noted. There is mild to moderate thinning of the central weight bearing cartilage with focal full-thickness delamination at the medial femoral condyle where there is mild marginal edema.
The Patellofemoral compartment is moderate thinning overlying the central and medial trochlear cartilage with an 8 mm near full-thickness cartilage defects. There is an additional full thickness cartilage fissuring at the median ridge of the patella spanning 3 x 6 mm with a nondisplaced cartilage flap.
Muscle/tendon, the periarticular muscles are maintained. The imaged tendons, inclusive of the extensor mechanism, are intact. Joint fluid: There is a small-moderate joint effusion. No popliteal cyst is seen. There are no intra-articular ossific loose bodies. Mild anterior subcutaneous edema is noted.
The neurovascular structures demonstrate normal course. Partial anterior lateral meniscus tear. Moderate medial compartment cartilage wear. Tricompartmental cartilage wear with full-thickness loss most notably at the patellofemoral compartment where there is a 6 mm nondisplaced patellar cartilage flap.
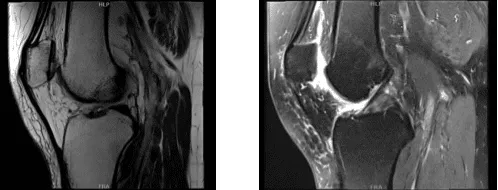
MRI-3T Right knee non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, nonhealing, injury to adjacent nerves and vessels, need for repeat surgery, need for rehabilitation and possible knee replacement in future.
We discussed systemic complications including blood clot, cardiac, pulmonary, neurological complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. The patient was put on a well-padded operating table. Right lower extremity was prepped and draped aseptically in a usual fashion. Time-out was called. Preop antibiotic was given.
Tourniquet was inflated upon exsanguination. Lateral entry portal was made through a parapatellar incision. Arthroscope was entered. Arthroscope was moved from the patellofemoral joint into the medial compartment. A spinal needle was used to make a medial portal. A high medial portal was made for access to the lateral compartment.
Examination of the knee was performed which showed a tear of the lateral freeing margin of the medial meniscus as well as tear of the medial freeing margin of the lateral meniscus along with discoid lateral meniscus. The ACL was intact. Meniscectomy was performed with the use of biters and shavers.
Saucerization of the lateral meniscus was also confirmed. The root as well as the periphery of the medial and lateral meniscus were intact. The ACL was intact.
Examination of the patellofemoral joint showed grade 1 to grade 2 arthritis on the lateral facet of the patella as well as grade 3 to grade 4 arthritis of the trochlea. Chondroplasty of the patella as well as trochlea was performed with the use of shaver and Coblation wand. Final pictures were taken and saved.
The knee was thoroughly irrigated and drained. Closure was done with # 4-0 nylon. Then, 20 cc of 0.5% Naropin mixed with 40 mg of Depo-Medrol was Injected into the knee. Dressing was done using Adaptic, 4 x 4, Webril, and Ace wrap. The patient was extubated and moved to recovery in a stable condition.

Intraoperative images
The patient seen by the doctor two weeks after the surgery for her post operative consultation, the patient has denied fever, pain, chills. She is WBAT without aid or limping. After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the knee.
We went over the arthroscopic pictures and removed the stitches visits. We will continue with ice and elevation of the knee to decrease swelling and pain. We will continue to utilize early mobilization and mechanical prophylaxis to reduce the chances of a deep vein thrombosis.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications. We also discussed the risk and benefits and common side effects of taking these medications. The patient will be back in three weeks time to evaluate their progress.
After two months the patient visits the office for her follow up checkup, the patient is not using crutches, her pain has improved and she is not limping. With the continued follow up checkup the patient showed progress from time to time she visits the office. She gets well after the surgery and with the help of continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
