This might involve fixing damaged muscles or tendons in the shoulder or cutting off bone spurs that are putting pressure on it. Arthroscopy, open surgery, or a combination of the two are surgical procedures that can be used to treat a rotator cuff injury.
Rotator cuff issues may worsen if left untreated, whether it be through rest, therapy, or surgery. Your discomfort can increase with time. Your shoulder’s strength and range of motion might deteriorate, making it more difficult to carry out normal tasks.
A 50-year-old patient was in our office with complaints regarding bilateral shoulder pain and neck and upper back pain. She has a history of neck injury. For aggravating factors, lifting, pushing/pulling, and throwing.
For associated symptoms, weakness, numbness, tingling, and pain with motion but reports no swelling, no redness, no warmth, no ecchymosis, no catching/locking, no popping/clicking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness. For location, bilateral (shoulder/back). For quality, aching, burning, and throbbing. For severity, she reported moderate.
The patient presented MRI results for both shoulders. For the right, low-grade interstitial tear of the posterior supraspinatus tendon. Mild supraspinatus and subscapularis tendinosis.
For the left, A low grade interstitial tear of the posterior supraspinatus tendon on mild background tendinosis. Tearing of the posterior-superior labrum. Mild acromioclavicular joint osteoarthritis.

MRI Left Shoulder Non-contrast
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections, and surgical options. I also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to infection, stiffness, damage to nerves and blood vessels, blood loss possibly requiring transfusion, blood clots, persistent or worsening pain, loosening or failure of implants, instability, tingling or numbness, anesthesia and systemic complications including cardiac, pulmonary, neurological complications and even death were discussed at length.
I also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
I talked about the possibility of not being able to alleviate all the discomfort. Also, I explained there is no guarantee all the function and strength will return. I discussed the type of implants that may be utilized during this surgery.
The patient expressed understanding of these risks and has elected to proceed with surgery. I discussed the patient’s medications and allergies and the possible need for medical and other clearances if needed. I have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome, and post operative protocol.
The patient was taken to the operating room where general anesthesia was induced. A supraclavicular block was given. The patient was put into the left lateral position with the right shoulder up. Preoperative antibiotic was given.
A posterior entry portal was made. The arm was put into flexion and abduction. Entry portal was made posteriorly to enter the glenohumeral joint. An anterosuperior entry portal was made under guidance of a spinal needle.
Examination of the joint showed a high- grade partial-thickness rotator cuff tear in the region of the supraspinatus. It also showed intact cartilage as well as labrum. Debridement of the rotator cuff tear was performed from the intra articular region.
The arthroscope was inserted into the subacromial region where debridement of the bursa was performed with the use of shaver. There was acromial spur, which was removed after use of Coblation wand, followed by a bur to remove the spurring. The CA ligament was released with the use of a Coblation wand.
The rotator cuff was found to be high- grade partial in the region of supraspinatus. Decision was made to repair the rotator cuff tear with the use of anchors and sutures. Footprints were developed and decorticated for healing to happen. A Healicoil anchor was inserted into the humeral head.
The tails of the suture were passed sequentially into the rotator cuff tear and tied over each other. A good repair was achieved. There was AC arthritis, which was cleaned with the use of Coblation wand and 1 cm of distal clavicle was excised with the use of a bur. Final pictures were taken and saved.
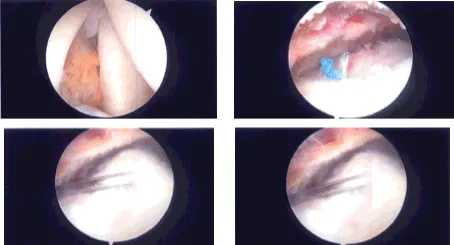
Intraoperative Arthroscopy Images
The shoulder was thoroughly irrigated and drained. Closure was done with the use of 3-0 nylon. Dressing was done with the use of Xeroform, 4×4, ABD, and tape. Shoulder immobilizer was applied. The patient was extubated and moved to recovery in stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on her shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
