Acromioplasty is a surgical technique that includes removing the acromion, a portion of the shoulder bone. The rotator cuff tendon, which supports and fortifies the shoulder joint, is impinged, thus surgeons perform the surgery to release it. Subacromial decompression and acromioplasty are synonyms.
The most frequent reason for shoulder discomfort is rotator cuff tendon impingement under the shoulder’s bony region. Inflammation or injury to the tendons occurs. The term rotator cuff tendinitis or bursitis is used to describe this ailment.
A 47-year-old patient was in our office with complaints regarding right shoulder pain due to a road traffic accident. For aggravating factors, lifting, twisting, and pushing/pulling. For quality, stabbing, sharp, and constant. For severity, she reported moderate. For timing, she reports cannot be identified.
For context, she reported cannot be identified. For alleviating factors, she reported nothing helps. For associated symptoms, no weakness, no numbness, no tingling, no swelling, no redness, no warmth, no ecchymosis, no catching/locking, no popping/clicking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness.
For previous surgery, none. The patient presented X Ray results that showed unremarkable radiographs of the bilateral shoulder.
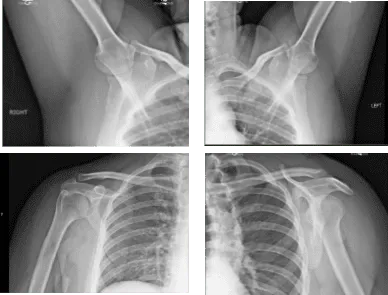
X-ray Bilateral Shoulders
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections, and surgical options. I also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to infection, stiffness, damage to nerves and blood vessels, blood loss possibly requiring transfusion, blood clots, persistent or worsening pain, loosening or failure of implants, instability, tingling or numbness, anesthesia and systemic complications including cardiac, pulmonary, neurological complications and even death were discussed at length.
I also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
I talked about the possibility of not being able to alleviate all the discomfort. Also, I explained there is no guarantee all the function and strength will return. I discussed the type of implants that may be utilized during this surgery.
The patient expressed understanding of these risks and has elected to proceed with surgery. I discussed the patient’s medications and allergies and the possible need for medical and other clearances if needed. I have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome, and post operative protocol.
The patient was taken to the operating room and supraclavicular block was given. General anesthesia was induced. The patient was turned to left lateral with the right shoulder up. She was positioned in a bean bag. All the bony prominences were well padded.
The right shoulder was prepped and draped aseptically in the usual fashion. Preoperative antibiotic was given. A posterior through the soft portal and arthroscope was inserted into the glenohumeral joint. Anterosuperior portal was made with the use of spinal needle.
Cannula was inserted into the anterosuperior portal. Examination of the glenohumeral joint showed no arthritis of the glenohumeral joint. Biceps was intact. There was tearing of the subscapularis tendon, which was debrided with the use of shaver.
There was a full-thickness tear through the anterior supraspinatus tendon, which was debrided with a shaver. The labrum was intact. Inferiorly the shoulder was intact. The arthroscope was inserted into the subacromial space where examination showed tear of the anterior supraspinatus tendon. Debridement of the subacromial bursa was done with the use of shaver.
Coblation wand followed by 6.0 burr was used to perform acromioplasty to remove the acromial spur and make space for further repair of the rotator cuff. The footprint of the rotator cuff was debrided with a use of Coblation wand followed by a shaver prepared for repair.
A double row SpeedBridge was planned. A lateral portal was made followed by. superior portal to insert the anchor. After visualizing the rotator cuff from the central portal and debriding it. The SwiveLock was loaded with FiberTape was planned to be inserted from the medial row.
Sponge was used over the footprint for the medial row and two SwiveLocks with FiberTape were inserted one anteriorly and one posteriorly. Each of the FiberTape was sequentially passed through the anterior and posterior rotator cuff tendons with full visualization and avoidance of the biceps’ tendon.
Now, the lateral entry of the SpeedBridge was planned with the arthroscope to the posterior portal. The punch was used to mark the insertion point on the anterior followed by posterior SwiveLock. Sutures were loaded on the SwiveLock for anterior and posterior sequentially and inserted and a good repair was achieved.
There was a dog ear, which was further repaired with the use of four sutures from the SwiveLock of the lateral row. A good repair was achieved, and good opposition was achieved. Completion of the acromioplasty followed by use of Coblation wand and a burr was done over the distal clavicular excision. About a centimeter of distal clavicle was excised with the use of a burr.
The shoulder was thoroughly irrigated and drained. Closure was done with the use of # 3-0 nylon. Dressing was done with a use of Xeroform, 4 x 4, ABD. The patient was put in a shoulder immobilizer. The patient was extubated in the recovery in a stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder.
Patients regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on her shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
