As we get older, we are prone to having pain, especially on our knees. Based on study, knee pain started to kick in in our 30s. Knee pain is mostly experienced by elderly people. The study presented below showed that elderly people get knee pain easily when they get older knowing no exposure to any injury.
Patient presented today is female with left knee pain for almost a month now. She started experiencing it with associated swelling and sharpness. She reports no injury. She is having radiating pain and weakness.
MRI results discussed and found out that there is moderate chondromalacia over the median ridge and medial facet of patella, with varying degrees of chondral surface fissuring and fraying.
Small joint effusion and lateral meniscus tear was also observed. By this time the patient decided to do rest and physical therapy and take naproxen and advised to return when no improvement happened.
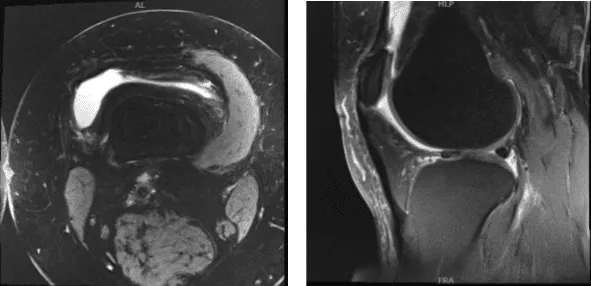
MRI – Right Knee Non-Contrast
After a month, the patient returned and mentioned no improvement happened after Physical Therapy. We discussed treatment options and the patient opted for surgical management.
We discussed risks and benefits including infection, nonhealing, repeat tear, need for repeat surgery injury to adjacent nerve and vessel, chronic knee pain, complex regional pain syndrome, deep vein thrombosis, systemic complications Ilka pulmonary embolism, cardiac and neurologic complications among others. The patient understood and signed informed consent.
The patient was taken to the operating room where she was placed on a well-padded operating table. General anesthesia was induced. Left lower extremity was prepped and draped in the usual fashion. IV antibiotic was given prior to the application of tourniquet. Aseptic prep and draping were performed. Time-out was called.
A lateral working portal was made through left-sided Incision. The scope was entered into a patellofemoral joint where arthritis was found on the medial and lateral facet of the patella as well as in the trochlea.
The scope was entered into medial femoral condyle where medial femoral condyle arthritis was found. There was a medial meniscus tear along the anterior body. The scope was entered into the intercondylar notch where ACL was Intact. The scope was entered into the lateral tibiofemoral Joint.
A horizontal flap tear of the right anterior margin of the posterior body of the lateral meniscus along with the medial fraying of the medial margin of the lateral meniscus was found. Medial entry portal was made with direct access to the lateral meniscus. The scope was entered and findings were reconfirmed.
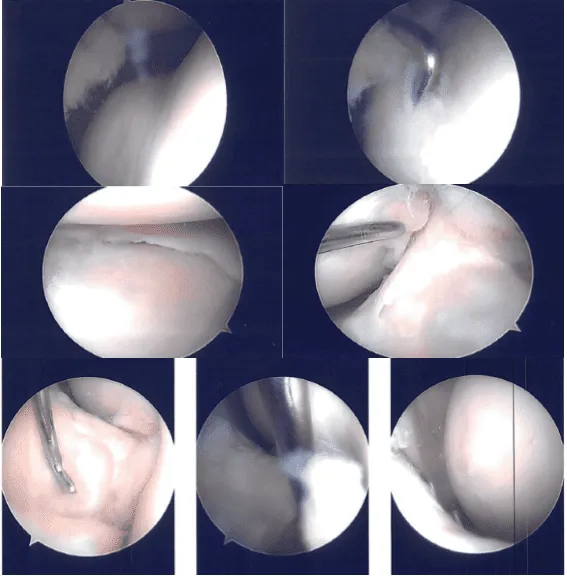
Intraoperative Images
The medial meniscectomy was performed using a shaver. Medial femoral chondroplasty was also confirmed using a shaver. Cyclops lesion was found on the ACL lateral Insertion. The cyclops was then excised using a shaver.
The scope was entered into the lateral compartment where the tears were reconfirmed. Excision of the medial horizontal flap was done using straight biter.
Cribbing of the lateral meniscus was done using a shaver. Balanced margins were achieved. There was no arthritis in the lateral femoral condyle. Now the attention was focused onto the patellofemoral joint.
Chondroplasty of the patellar medial and lateral facet as well as the trochlea was performed. There were grade 2 to grade 3 lesions. There was a medial shelf plica which was excised completely.
Final findings were checked and reconfirmed from the other portal also. The final pictures were saved. The knee was irrigated thoroughly. Closure was done using nylon #4-0.
Depo-Medrol 80 mg injection was injected into the knee. Dressing was done using 4 x 4, ABO, Webril, and Ace wrap. The patient was extubated and moved to the recovery unit in stable condition.
After four weeks post operative, the patient visited the office to check the status of the operation. She is doing well, has limp but able to manage. She is currently using ice and pain medications. Denies having fever or chills. The patient has been doing conservative treatment to her knee.
There is a full range of motion without discomfort. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. The patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
