When the knee’s anterior cruciate ligament (ACL) is overstretched or torn, this is referred to as an anterior cruciate ligament injury. Both partial and full tears are possible. A hinge joint called the knee is formed by the ligaments connecting the massive lower leg bone (tibia) and upper leg bone (femur).
Your knee may become extremely unstable and lose its entire range of motion if the ACL is torn. Certain motions, including turning immediately, may become challenging as a result. It could be impossible to play some sports.
The damaged ligament is removed during ACL repair and replaced with a tendon, a strip of tissue that typically joins muscle to bone. The donor tendon or another area of your knee is used for the tendon transplant.
A 51 year-old patient was in our office with complaints regarding instability of the right knee. He was at a shop, stepped on a puddle and slipped and fell hurting both knees and RT hip. For aggravating factors, standing, walking, twisting, upstairs, and downstairs.
For associated symptoms, weakness, swelling, and popping/clicking but reports no numbness, no tingling, no redness, no warmth, no ecchymosis, no catching/locking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness.
For location, left (knee) and right (knee & hip). For quality, aching, sharp, and frequent. For severity, severe. For timing, he reported recurrence. For context, he reported a fall. For previous surgery, he reports none.
The patient presented MRI results that showed mild to moderate insertional quadriceps and proximal patellar tendinosis. There is prominent spurring along the inferior pole of the patella without a separate ossific fragment or surrounding bone marrow edema indicative of previous traction injury.
No meniscal tear or ligament injury. Cartilage is preserved. For the right knee, the X Ray results have shown Shallow undersurface tear at the posterior horn/body junction of the medial meniscus and undersurface fraying of the posterior horn.
Mild quadriceps and patellar tendinosis without a tear. Mild prepatellar bursitis and moderate surrounding soft tissue edema. We discussed treatment with the patient. The patient had tried physical therapy in the past.
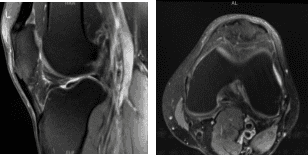
MRI-3T Left Knee non-contrast
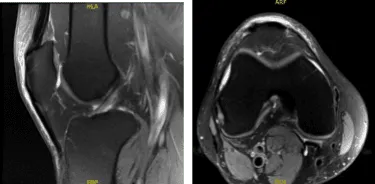
MRI-3t Right Knee non-contrast
We discussed treatment options and the patient was offered surgical management. We discussed the risks and benefits including infection, bleeding, injury to nerves and vessels, failure of surgery, rerupture of set and need for repeat surgery, arthritis, among other things.
We discussed systemic complications including blood clot, cardiac or pulmonary complications, among others. The patient understood and signed informed consent.
The patient was taken to the operating room where he was placed on the operating room table. The patient was sedated and the right knee was injected with 15 cc of 2% Marcaine and 15 cc of 2% Lidocaine and 15 cc of .5% Marcaine mixed with epinephrine for a local block. A tourniquet was applied. The patient was kept sedated during the procedure.
The right knee was prepped and draped aseptically in the usual fashion. A timeout was called. Preoperative antibiotics were already given. Esmarch was applied and the tourniquet was elevated. Lateral anterior portal was made with an incision and the arthroscope was inserted.
Medial anterior portal was made with the use of a spinal needle and knife. Examination of the medial femoral compartment showed horizontal and oblique tear of the lateral free margin along the body of the posterior hom. This was done with the use of straight biters and shavers.
Balanced margins could be achieved. Examination of the rest of the tibiofemoral compartment was good. Examination of the infrapatellar notch showed an intact ACL. Examination of the lateral tibial compartment showed intact meniscus.
There was Grade III medial injury to the articular cartilage which was debrided to balanced margins. The bone was then exposed. Examination of the patellofemoral compartment showed intact cartilage. Final pictures were taken and saved.
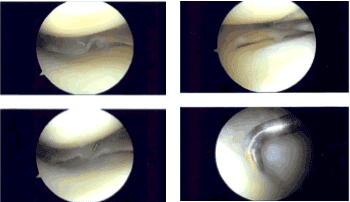
Intraoperative Arthroscopy Images
The knee was thoroughly irrigated and drained. Closure was done with the use of 4-0 nylon. Dressing was done with the use of Xeroform, 4 x 4s, ABD, Webril and ACE wrap. The patient was extubated and moved to the recovery room in stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on December 8, 2025.
