A torn meniscus cartilage in the knee can be treated with an outpatient, minimally invasive surgical technique called an arthroscopic meniscectomy. For four months following meniscus (cartilage) repair, patients are prohibited from twisting, pivoting, squatting, deep knee bends, or impact activities.
A 65 year-old male patient presents with left knee pain due to a car accident. He has tried to do Physical Therapy, chiro, NSAIDs but had no relief. An MRI of the patient’s knee revealed a medial meniscus tear in the left knee.
We spoke about our alternatives for treatment and decided on surgical treatment. Infection, bleeding, damage to nearby nerves and blood vessels, persistent knee discomfort, the need for revision surgery, and the requirement for knee replacement in the event of fusion were just a few of the risks and advantages we covered.
We also talked about systemic issues such as blood clots, cardiac, pulmonary, neurological, and fatal issues. The client was aware and gave informed consent.
The patient was taken to the operating room where he was placed over a well-padded operating room table. General anesthesia was induced. The left lower extremity was prepped and draped aseptically in the usual fashion after application of thigh tourniquet.
Preoperative antibiotics in the form of 2 g Ancef was given. Tourniquet was elevated to 350 mmHg and 25 minutes of tourniquet time was used for the surgery. Time-out was called.
A lateral arthroscopic entry portal was made. Arthroscope was inserted and examination of the patella showed intact cartilage. Examination of the medial compartment showed fraying of the medial meniscus.
The medical entry portal was made with the use of a spinal needle. near full thickness. Partial medial meniscectomy of the left knee was performed with use of biters and shavers.
Balanced margin of medial meniscus was achieved. Examination of the intercondylar notch showed intact, intact lateral meniscus as well as cartilage. The cartilage of the medial tibiofemoral compartment was also intact.
Examination of the patellofemoral joint was again done which showed grade 4 lesion of the trochlea. Abrasion chondroplasty with excision of the frayed margins of the cartilage and balancing margins were performed with the use of shaver. The final picture was taken and saved.
The knee was thoroughly irrigated and drained. Closure was done with the use of #3-0 nylon. Marcaine 0.5% 18 cc mixed with 40 mg of Depo-Medrol was injected into the knee. Dressing was done with the use of 4 x 4s, ABD, Webril, and Ace wrap. The patient was extubated and moved to the recovery unit in a stable condition.
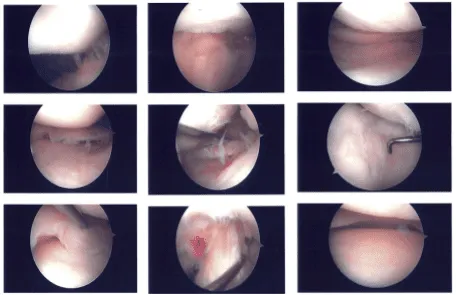
Intraoperative images
The patient went to the office for his one week post operative consultation, no x-rays were needed, he denies fever and chills, his pain is well controlled. After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the knee.
We went over the arthroscopic pictures and removed the stitches during the visit. We will continue with ice and elevation of the knee to decrease swelling and pain. We will continue to utilize early mobilization and mechanical prophylaxis to reduce the chances of a deep vein thrombosis.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications.
We also discussed the risk and benefits and common side effects of taking these medications. The patient’s follow up checkup will be regular every three weeks’ time to evaluate the progress.
The patient did well after the surgery without taking physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
