The patient is a 60-year-old female with complaints of left knee pain for the past 5 years.. The pain is moderate in intensity. She got a cortisone injection 6 months ago and has been improving since then till last month when the pain started again.
The patient describes the pain as stabbing and throbbing The pain is constant and does in sleep. The pain is associated with twisting or bending. The problem has been getting better since it started. Bending and lifting make the pain worse lying down make the symptoms better. She works at a laundry service and has a lot of kneeling and crawling.
The patient is right-handed. The pain has severely affected her day to day activities and work.
The patient is a non-smoker. The patient is currently not taking any medications. The patient reports no allergies.
On general physical examination, the patient is calm conscious cooperative, and well oriented to time place and person. The gait of the patient was steady and antalgic. Upon examination of the left knee, there is tenderness on palpation along the medial joint line and has no effusion. The patient also has patellofemoral crepitus and there is no tenderness on palpation along the medial and lateral patellofemoral joint line.
The patellar grinding test is negative. The patient has no discomfort with McMurray’s maneuvers, and the knee is stable. They have full flexion and extension. Bilateral lower extremities have 5/5 strength and are neurovascularly intact distally. There are no erythema, warmth, or skin lesions present.
On examination of the contralateral extremity, the patient is non-tender to palpation and has an excellent range of motion, stability, and strength.
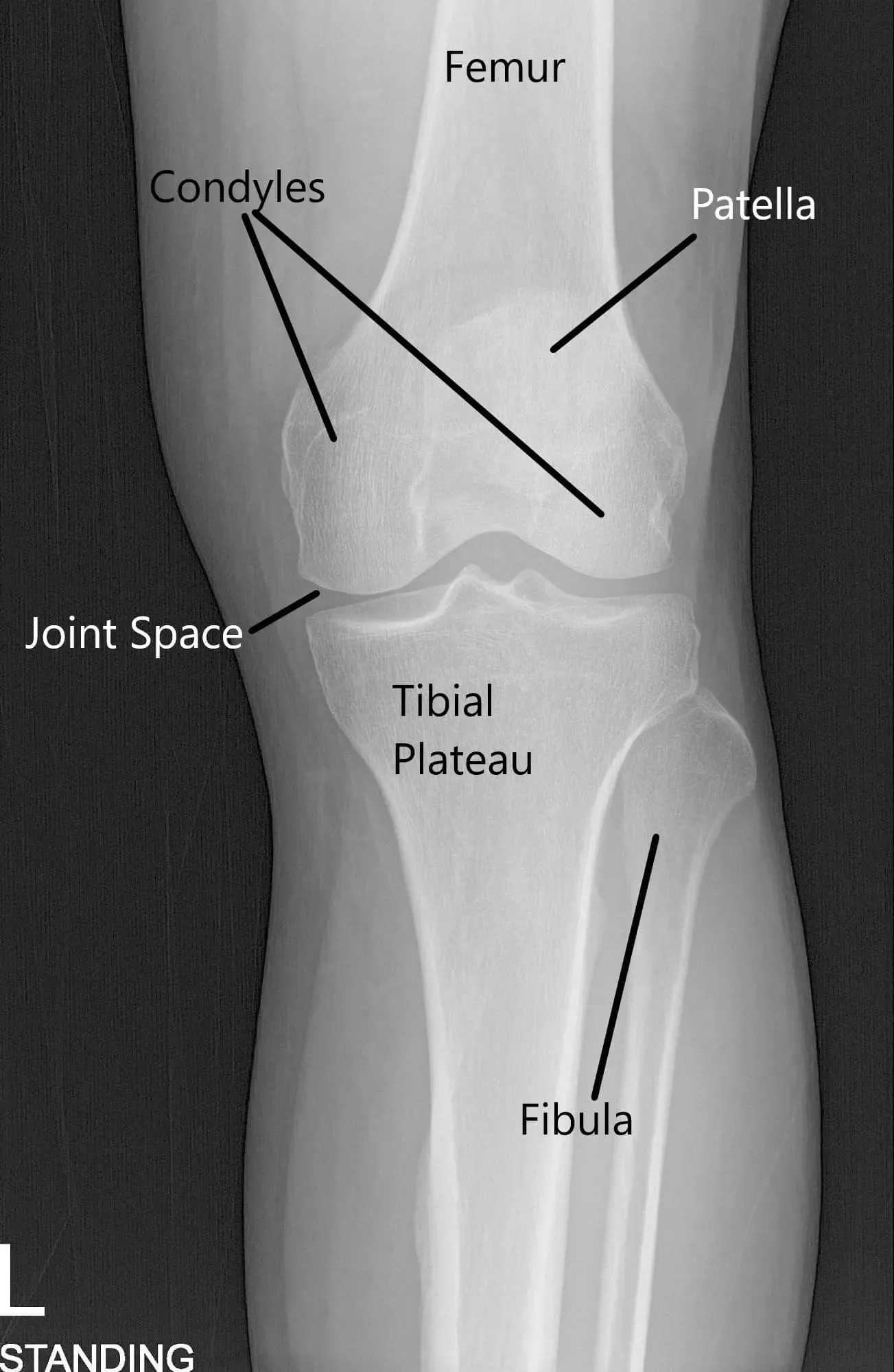
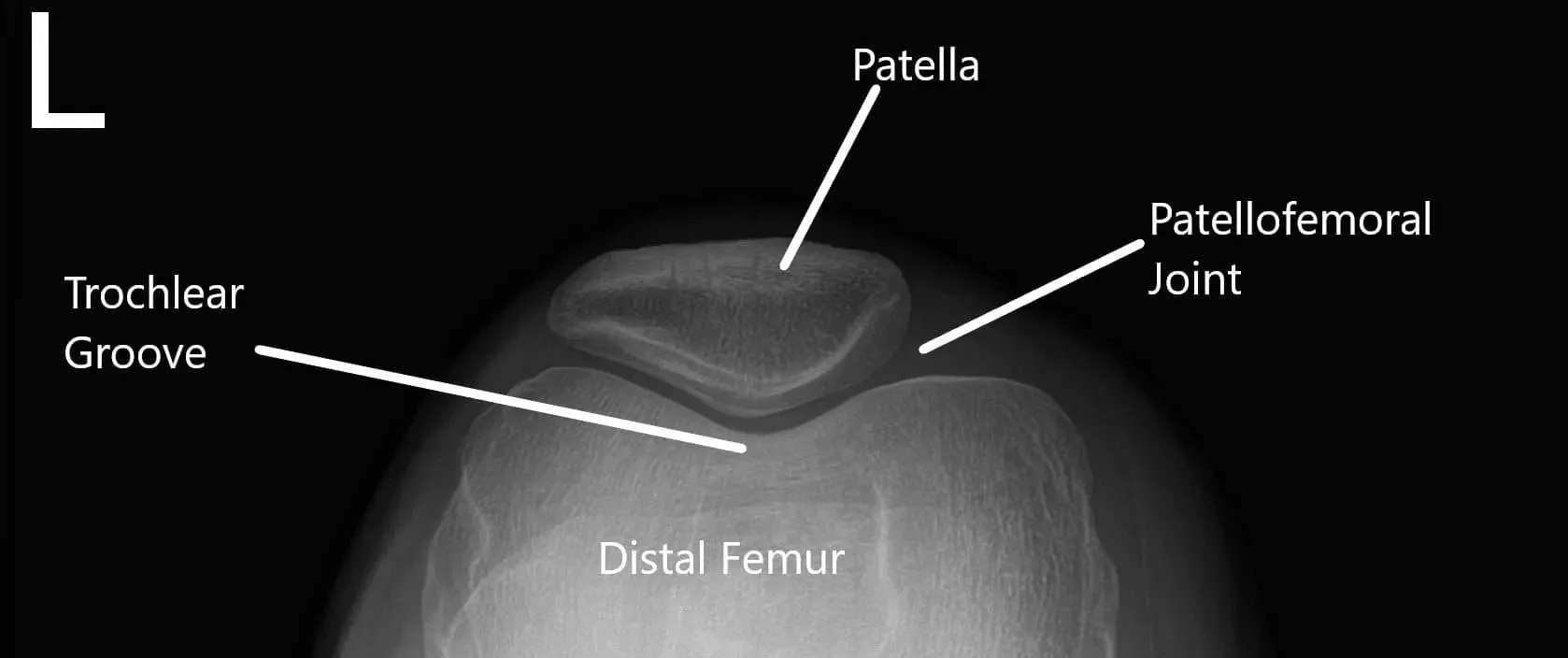
X-ray of the knee in AP and skyline view.
MRI of the left knee suggested tear of the posterior horn and posterior horn/body segment junction medial meniscus, with mild meniscal extrusion into the medial gutter and mild chondromalacia patella.
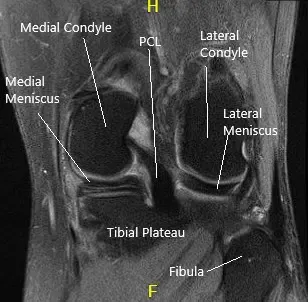
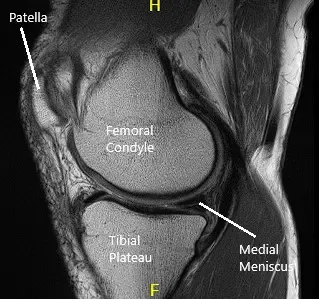
MRI of the knee in sagittal and coronal sections
We discussed the treatment options for the patient’s diagnosis, which included: living with the extremity as it is, organized exercises, medicines, injections, and surgical options. We also discussed the nature and purpose of the treatment options along with the expected risks and benefits. The patient has expressed a desire to proceed with surgery.
The patient was educated regarding the inherent and unavoidable risks which include, but are not limited to: anesthesia, infection, damage to nerves and blood vessels, blood loss, blood clots, and even death were discussed at length.
The patient expressed an understanding of these risks and has elected to proceed with the surgery.
PREOPERATIVE DIAGNOSIS: Medial meniscus tear, left knee.
POSTOPERATIVE DIAGNOSES: Medial meniscus tear left knee and Grade 4 osteochondral damage, patella.
SURGERY PERFORMED: Partial medial meniscectomy, Microfracture of Patella Left knee
PROCEDURE: The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. Tourniquet was put on the lower thigh on the left side. The left knee was put into a knee holder.
Aseptic prep and draping were performed. A timeout was called. The preoperative antibiotic was given. The tourniquet was inflated. Lateral entry portal was made and the scope was entered. Osteochondral grade 3 to grade 4 damage was found on the lateral inferior patella. A lot of debris was found in the knee as well as in the suprapatellar pouch and medial gutter.
The knee scope was moved to the medial compartment where a lot of debris as well as medial meniscus tear could be seen. A medial entry portal was made. A probe was entered and meniscal tear was examined and the picture was taken. A shaver was inserted to clean off the debris as well as margins on the medial meniscus. Straight as well as up going as well as the left-sided punch was used to clean the meniscus and remove the ragged margins.
The medial meniscus was balanced on the body to the posterior horn as well as to the posterior root. Now the knee scope was entered into the intercondylar area where ACL was found to be intact. The scope was directed towards the lateral meniscus where debris was present. The shaver was used to remove the debris.

Intraoperative arthroscopic images.
The lateral meniscus was found to be intact. The scope was moved to the patellofemoral joint where the patellar lesion was debrided. The wound was exposed. The lateral gutter was found to be clean. Now, the scope was removed and inserted from the medial portal.
The shaver was introduced from the lateral portal. The final balancing of the medial meniscus was performed. The lesion was also debrided. Microfracture of the patellar osteochondral defect was done using pigtail punches and subchondral fat globules could be seen from the microfracture sites. Final pictures were taken and saved.


Intraoperative arthroscopic images.
The wound was lavaged using a copious amount of normal saline. The scope was removed. The closure was performed using #4-0 nylon; 20 ccs of 0.5% ropivacaine was injected into the knee. The dressing was done using Adaptic, 4×4, and ABD along with web roll and Ace wrap. The tourniquet was released.
The patient was extubated and moved to the postoperative care unit in a stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
