The shoulder is one of the most mobile joints, it is more vulnerable to injury. It is a relatively shallow ball and socket joint found between your upper arm’s big bone (humerus) and your shoulder blade (scapula).
Arthroscopy is a powerful test for evaluating and treating shoulder joint problems. Arthroscopy is a surgical technique that inserts a small telescope-like equipment (arthroscope) and other tools into the shoulder through small incisions (cuts made by the surgeon).
A 42 year-old male patient visits the office with complaints of right shoulder pain. The patient went to the office to ask for a second opinion. He states that the pain started two weeks ago and he was unsure how it happened.
He is a sergeant for the NYPD. Upon the examination, we agreed to take an MRI to see what was the real cause of his pain.
MRI were reviewed and discussed by the doctor, there is mild supraspinatus and infraspinatus tendinosis. Mild subscapularis tendinosis is present with a focal partial-thickness tear of the mid fibers.
A small lobulated hyperintense focus along the superficial margin of the subscapularis tendon likely reflects a small ganglion. The tree’s minor tendon is intact. No full-thickness rotator cuff tear is identified. No disproportionate rotator cuff muscle atrophy is present.
There is mild acromioclavicular joint arthrosis. Mild subacromial-subdeltoid bursitis is present. It showed that it has partial tearing of the rotator cuff as well as tear of the biceps tendon along with subacromial spur and AC arthritis. The biceps tendon is located within the bicipital groove.
There is mild biceps tendinosis, preferentially of its intra-articular portion, with a linear partial-thickness tear of the intra-articular portion of the bicep’s tendon extending distally to the level of the proximal bicipital groove. Minimal biceps tenosynovitis is present
There is a tear of the superior labrum which extends into the anterior superior and posterosuperior labrum. No focal chondral defect is identified over the glenohumeral joint. Trace fluid is present within the glenohumeral joint. There is no acute fracture or osteonecrosis.
Mild multifocal rotator cuff tendinosis with a focal partial-thickness tear of the subscapularis tendon. No full-thickness rotator cuff tear. Linear partial-thickness tear of the intra-articular portion of the bicep’s tendon extending distally to the level of the proximal bicipital groove, superimposed on mild tendinosis, with minimal biceps tenosynovitis.
Tear of the superior labrum which extends into the anterior superior and posterosuperior labrum. Mild acromioclavicular joint arthrosis. Mild subacromial-subdeltoid bursitis.
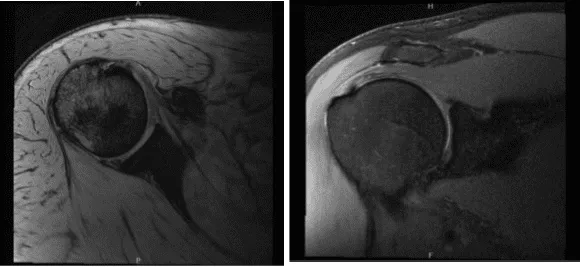
MRI-3T Right shoulder non-contrast
During the visits, we discussed treatment options and the patient opted for surgical management.
We also discussed the risks and benefits and complications including bleeding, infection, nonhealing, need for rehabilitation, need for repeat surgery, weakness, injury to adjacent nerves and vessels, systemic complications including blood clot, cardiac, neurological, pulmonary complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was then introduced. He was put in the left lateral position with the right shoulder up. The right shoulder was prepped and draped aseptically in the usual fashion. He was held in a lateral position with the use of a beanbag.
All the bony prominences were well padded. The right arm was draped and put into traction of 10 pounds in 45-degree abduction and traction. Time-out was called. Preoperative antibiotic was given. Posterior entry portal was made. Arthroscope was inserted into the glenohumeral joint.
Examination of his glenohumeral joint showed tendinosis of the biceps tendon. It also showed sub labral holes and the Buford complex. There was labral degeneration.
There was an articular sided rotator cuff tear of the supraspinatus and infraspinatus. Anterior entry portal was made using the single stick. Shaver was introduced and labrum was debrided. A biter was used to cut the biceps tendon.
There was an additional capsular reflection attached to the glenoid labrum, which was merged with the adjacent capsule. It seemed like a bicep’s tendon, but was not distinct. Debridement was done to relieve it from the superior labrum. Examination of the shoulder joint did not show any abnormality.
The arthroscope was entered into the subacromial space. Bursitis was there. A shaver was entered from the anterior portal and bursa was excised. A lateral entry portal was made. Cannula was inserted. Further dissection was performed.
The rotator cuff was examined and found to be thinned out with no complete tear. It was decided to supplement the rotator cuff with the use of a Regenstein implant. Acromioplasty was performed with the use of coagulation followed by burr. AC arthritis was identified.
CA ligament was released and acromioplasty was completed. AC joint was also debrided using coagulation followed by burr. Distal clavicular excision was done from the posterior followed by the anterior portal using the burr and 1 cm of distal clavicle was excised. Pictures were taken.
The Regenstein implant was brought in and inserted through the lateral portal. It was held over the rotator cuff. Separate entry portal was made superiorly for the PLA tacks to go Sweep was inserted and PLA suture tacks were inserted sequentially on the borders of the Regenstein w. with the use of PLA anchors (W.2). The implant was found to be well seated and fixed. Picture was taken and saved. The shoulder was thoroughly irrigated and drained.
Now, one of the Fiber Loop threads was passed through the bioabsorbable screw and it was inserted neocortical over the tendon and fixed. The loose sutures were tied on to each other again. Achieving good fixation, the wound was thoroughly washed, pictures were taken.
Closure was done in layers using #0 Vicryl and #2-0 Vicryl and Monocryl. Arthroscopic incision was closed with nylon. Dressing was done using 4 x 8, ABD, and tape. The patient was put in a shoulder immobilizer. The patient was extubated and moved to a recovery unit in stable condition.
The patient saw the office for his one week post operative visit. The patient is doing well after the surgery, his status post right shoulder arthroscopic debridement, acromioplasty, distal clavicle excision and mini open biceps tenodesis.
The pain has improved and he denied chills and fever, no swelling, tenderness, or warmth and wound clean and dry, appropriate range of motion, and neurovascular intact.
After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. We went over the arthroscopic pictures and removed the stitches during the visits.
We advised him to continue with ice and elevation of the shoulder to decrease swelling and pain. We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications.
We also discussed the risk and benefits and common side effects of taking these medications. After a month of taking the treatment, the patient’s progress has not been denied, he is not using any sling and the pain has improved.
Just because of the follow up checkup the patient showed progress from time to time he visits the office. With the continued follow up checkup the patient showed progress from time to time he visits the office. He gets well after the surgery and with the help of continuing physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
