The human shoulder is said to have the largest range of motion in the entire body. Our shoulder muscles enable us to rotate, flex, extend, and abduct.
According to research, rotator cuff tears, frozen shoulders, and instability are the three most prevalent injuries to the human shoulder. This article will discuss rotator cuff tears. A rotator cuff tear left untreated could result in lifelong loss of mobility.
The patient is complaining of lower back, neck, and left shoulder pain when they arrive at our office. The patient recalls suffering injuries in a car accident. The level of the pain ranges from very severe.
According to the patient, the pain is piercing, stabbing, agonizing, and scorching. The pain is ongoing and does not keep me up at night.
The discomfort is accompanied by weakness and radiating pain in the left leg. The symptoms are aggravated by standing, lifting, resting in bed, bending, and sitting. Icing and resting help with the symptoms.
Since the beginning, the issue has only become worse while remaining unchanged. She hasn’t been able to work since the accident.
There is no discernible shoulder girdle atrophy on a left shoulder examination. There are no ecchymosis, abrasions, lacerations, or soft tissue swelling. The shoulder’s active range of motion is constrained. The amount of active ROM is limited.
I can passively move the arm almost completely in all directions. The patient exhibits a Hawkins sign and an impingement that is clearly positive. At forward flexion and lateral abduction, the strength of the rotator cuff is reduced by 3/5.
Additionally, the patient has weakness in external rotation. The joint has no creaking sounds. The AC joint cannot be palpated to generate pain, and cross-body adduction does not cause any discomfort.
Strength of the extremities is comparable to the contralateral side and is 5/5 when the biceps, triceps, and wrist are extended. DTRs are symmetrical and intact at +2/4.
Full cervical range of motion is present, and there is no discomfort when the paraspinal musculature or medial scapular boundary are palpated. Spurling’s indication is adverse.
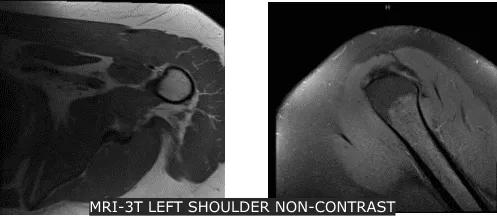
Xray were reviewed and discussed that his left shoulder showed normal radiographs. Advised patient to take MRI for us to see the reason behind and found out partial thickness tear of the subscapularis tendon though there is no high-grade partial or full thickness rotator cuff tear. Presence of supraspinatus and infraspinatus tendinosis.
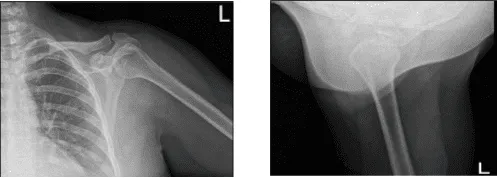
Left Shoulder X-ray
We discussed surgical and non-surgical treatment and patient agreed to try first the non-surgical like injection of cortisone, elevation, rest and taking OTC anti-inflammatory medication.
Patient also added that she finds pain physician. But after few weeks patient returned in our office for non-surgical treatment help her temporarily.
Patient opted for surgical management.
We discussed risks and benefits of surgery, including infection, nonhealing, need for repair, rehabilitation, possibility of decreased suboptimal result, need for repeat surgery, need for rehabilitation and physical therapy, need for cortisone injection in the future, systemic problems including injury to adjacent nerves and vessels; systemic problems including blood clot, cardiac, neurological, pulmonary complications and even death.
The patient understood and signed an informed consent.
The patient was brought into the operating room to receive a brachial block. Anesthesia was induced throughout. The patient’s left shoulder was raised while they were positioned laterally.
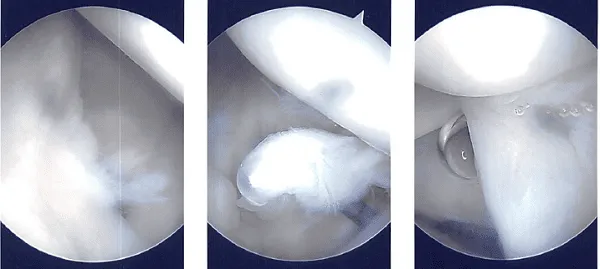
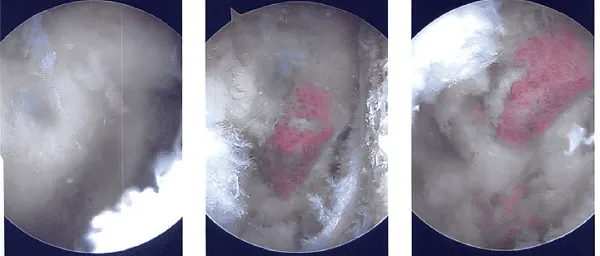
A beanbag held the position, and all of the bone prominences were well-padded. Behind the posterolateral corner of the acromion, a surgical incision was made. The glenohumeral joint was penetrated with the scope. There was a glenohumeral joint examination.
The labral hole was present. Labral degenerations were removed by shaving. The posterior labrum had degeneration, which was cleared out by shaving. There was subacromial bursitis.
Using a shaver, a thorough bursectomy was performed. It was created a lateral portal. The acromion was frayed and had a type 2 (curved configuration) configuration.
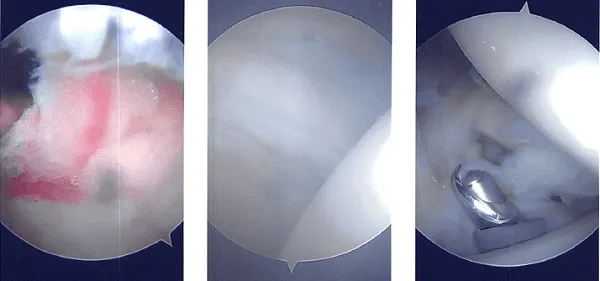
Acromioplasty was decided upon. After cleaning with a heat wand and a bur, acromioplasty was carried out. The AC joint was checked after a comprehensive acromioplasty and found to be degenerating. Excision of the distal clavicle was planned. The distal clavicle was removed using a wand and then a bur.
The distal clavicle’s last centimeter was removed. Final images were captured and stored. Nylon #4-0 was used for closure. After being extubated, the patient was taken to the recovery area.
The dressing procedure involved the use of Adaptic 4 x 4 ABD tape. An immobilizer for the shoulder was applied to the patient.
After a week post-operative, patient came in the office discuss the treatment options. We have decided to proceed with formal physical therapy as well as home exercise program for the rehabilitation of her shoulder. Stitches were removed.
Patient will continue the ice and elevation for it helps on her condition. Patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
