The shinbone (tibia) is covered with thick, springy bands of cartilage called the medial and lateral meniscectomy. They support the knee and serve as shock absorbers. Size and severity of meniscus tears can vary greatly.
Debilitating chronic joint pain is possible. Simple actions like sitting in a low chair or climbing a flight of stairs might become difficult. Additionally, you can experience discouragement if you can’t engage in your preferred activities or sports.
A 57-year-old patient was in our office with complaints regarding right knee pain. He tried physical therapy as well as anti- inflammatory medications, which did not help. He got an MRI done, which showed complex medial meniscus tear.
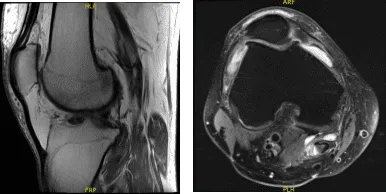
MRI Right Knee Non-contrast
We discussed the treatment options and opted for surgical management. We discussed the risks and benefits including infection, bleeding, injury to the adjacent nerves and vessels, failure of surgery, need for repeat surgery, possible total knee replacement in the future among others.
We discussed systemic complications including blood clots, cardiac, pulmonary, neurological complications among others. The patient understood and signed the informed consent.
The patient was brought to the operating room where he was placed on the well-padded operating table. General anesthesia was induced. A tourniquet was placed on the right thigh. The tourniquet was elevated to 325 mmHg and about half an hour of tourniquet time was used for the surgery.
A lateral entry portal was made. Examination of the medial tibial and femoral compartments showed grade 3 to grade 4 arthritis of the medial femoral and tibial condyle. There was a tear on the medial meniscus, which was cleaned. The medical entry portal was made with the use of a spinal needle.
The medial meniscus was cleaned with the use of shaver and biter. Balanced margins were achieved. The cartilage of the medial femoral condyle was also shaved with the use of a shaver. Examination of the intercondylar notch showed intact ACL.
Examination of the lateral compartment showed meniscus tear in the posterior horn along with grade 3 to grade 4 arthritis changes of lateral tibial and femoral condyle. The meniscus was shaved with the use of a shaver along with cleaning of the cartilage of the lateral femoral and tibial condyles.
Examination of the patellofemoral condyle showed grade 3 to grade 4 changes of the trochlea, which was cleaned with the use of a shaver again. The patella also showed grade 1 to grade 2 of cartilage changes which were also cleaned. The knee was already irrigated and drained.
Closure was done with the use of 3-0 nylon. Then, 30 mL of Marcaine mixed with 40 mg of Depo-Medrol was injected into the knee. The dressing was used with the use of 4×4, ABD, Webril and Ace wrap. The patient was extubated and moved to Recovery in stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
