Your elbow is made up of a number of crucial joints that are located between your upper arm and wrist. Your radial head is shaped like a disk and allows you to straighten your arm and elbow out while moving your wrists from a palms-up to a palms-down position. It is essential to many limb motions.
A group of ligaments surround the elbow joints, supporting your arm and preventing it from flopping. An elastic band of tissue known as a ligament binds bones together. As a result, your elbow isn’t well shielded and is vulnerable to harm like radial head fractures.
This fracture typically results from falling onto extended palms. A proximal radius fracture can occur, for instance, if you fall off a scooter, skateboard, or monkey bar, or if you are hit hard in a contact activity like football, lacrosse, or hockey.
Patient is a 26 yr old male, right hand dominant with complaints of pain in the right elbow. He recalls suffering an arm injury while playing soccer. When he fell, he had a deformity, which was pushed back by tugging.
The patient characterizes the pain as throbbing, stabbing, and sharp, and it also interferes with his sleep. Numbness, tingling, and puffiness are related to it. The sensations get worse when he twists and lie in bed.
The patient rests upright while being examined at the right elbow. Over the lateral face of the radial head, they are palpably tender. Place the brace after. They are neurovascularly intact distally and have 5/5 power.
No erythema, warmth, or cutaneous lesions are visible. The patient has a good range of motion, stability, and strength upon examination of the contralateral extremity, and is not tender to palpation.
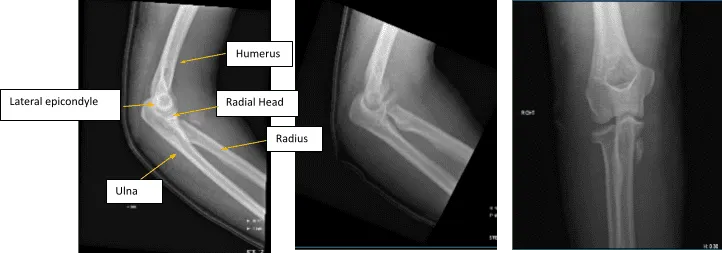
Figure 1. AP Oblique and Flexion Lateral Projection of Right Elbow
Hemarthrosis and a comminuted, affected, acute radial head fracture is present. The plantar-medial portion of the proximal shaft of the right ulna is home to a fracture fragment that has been severely misaligned. Though no donor defect is visible, this could be a fragment of the radial head that has been significantly displaced. A second fracture site is also a possibility.
We talked about the patient’s diagnosis and the therapy choices, which included managing the extremity as it is, structured exercises, medications, and surgical options. Along with the anticipated risks and benefits, we also talked about the nature and purpose of the available treatment choices.
The patient has indicated that he wants to have the procedure. I talked at length with the patient about the risks that are inherent and inevitable, including anesthesia, infection, damage to the nerves and blood vessels, blood loss, blood clots, and even death. We also discussed the potential inability to resume previous activities or work, the requirement for additional surgery, and complex regional pain syndrome.
The patient is also aware that a protracted rehabilitation process usually follows a surgical operation. We discussed the prospect that not all of the discomfort could be relieved. Also, there is no guarantee all the function and strength will return. The patient also understands the risks of re-tear or failure to heal.
The patient understands implants may be utilized during this surgery. The patient has decided to go ahead with the surgery despite acknowledging these dangers. We’ve talked about the surgical approach (radial head fixation vs. excision) as well as reasonable hopes for the risks, result, and postoperative instructions.
Brachial block was performed. The patient’s splint on the right upper extremity was removed and a tourniquet was applied on the upper arm. The right upper extremity was cleaned with chlorhexidine scrub followed by chlorhexidine paint and allowed to dry for 3 minutes.
A stockinette was put on after aseptic painting and the right upper limb was draped. Ioban was applied after marking the skin for the cut. After limb exsanguination with an Esmarch bandage, the tourniquet was stretched to 250 mmHg.
An incision was made straight over the lateral epicondyle, along the posterior lateral aspect of the elbow joint, and all the way to the shaft of the radial bone using Kocher’s approach.
The annular ligament was opened with sharp dissection. The radial head fragment, which was located far medially, was tried to locate through the injury interval along the anterior border and anterior surface of the radius.
The radial collateral ligament was already injured and partially avulsed. The lateral epicondyle and the remaining of the lateral collateral ligament along with the common extensors were elevated with sharp dissection from the lateral epicondyle to make more exposure for the fracture.
The fracture fragment was delivered through the anteromedial incision. The radial head which was lying in a tilted position was corrected and this led to completion of the fracture and the remaining part of the head of the radius could be delivered out of the elbow joint.
The two fragments of the radial head were fixed together and held by a K-wire and were fixed using a headless Acutrak-2, 20 mm x 2.4 mm screw which was buried down to the bone.

Figure 2. Image of Elbow with 3 cortical screws
A proximal radius plate of appropriate contour was fixed to the radial head using two locking screws. One of the anterior locking screws was passing through the intraarticular fracture site and allowed compression. The head of the radius and the plate was delivered into the wound and aligned with the shaft found to be acceptable and was provisionally fixed with the K-wire.
The plate was fixed to the distal fragment using 3 cortical screws (Figure 2). One more locking screw was passed into the head. No bone gap was found in the fracture site. The patient tolerated the procedure well. The patient was moved to the postoperative care unit in stable condition.

The patient undergo X-ray every week to monitor the progress of the elbow radial fracture. Postsurgical changes at the radial head are noted with satisfactory position of the hardware. In the second week, can notice the Stable postsurgical changes involving the proximal radius.
Third week post saw the repair of a complex fracture of the proximal radius in a good position fixed with plate and screws. After a month, early healing of the surgically treated comminuted radial head fracture is noted.
We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. The patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
