Meniscectomy, a kind of arthroscopic knee surgery, is the term used to describe the surgical excision of a torn meniscus. Your meniscus acts as a knee cushion and balances your weight to keep your knee stable.
Knee arthroscopy frequently involves the surgical treatment known as arthroscopic chondroplasty. Chondroplasty is specifically done to smooth out damaged cartilage in the knee to minimize friction in the joint. If the cartilage is only mildly to moderately worn, it is an option.
A 48-year-old patient male presents bilateral knee pain, left Rt. He has been seen by another doctor and he is here for a second opinion.
Degeneration of the medial meniscus with a horizontal tear involving its body. Tricompartmental degenerative changes, most pronounced in the medial femorotibial compartment. Moderate knee joint effusion.
MRIs were reviewed and discussed by the doctor; We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections and surgical options.
We also discussed the nature and purpose of the treatment options along with the expected risks and benefits. The patient has expressed a desire to proceed with surgery, and we think that is a reasonable option.
We educated the patient regarding the inherent and unavoidable risks which include, but are not limited to: infection, stiffness, damage to nerves and blood vessels, blood loss possibly requiring transfusion, blood clots, persistent or worsening pain, loosening or failure of implants, instability, tingling or numbness, anesthesia and systemic complications including cardiac, pulmonary, neurological complications and even death were discussed at length.
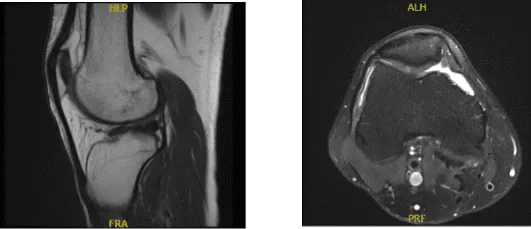
MRI Right Knee non-contrast
The patient was taken to the operating room where general anesthesia was induced. Left eye was prepped and draped aseptically in usual fashion. A low thigh tourniquet was applied. Preop antibiotic was given. Time-out was called. Tourniquet was elevated. Lateral entry portal was made.
An arthroscope was inserted. A medical entry portal was made with the use of a spinal needle. Examination of the medial tibiofemoral compartment showed a tear of the medial meniscus in the posterior horn. Also showed grade 3 to grade 4 osteoarthritic lesions in the medial tibial plateau as well as femoral condyle.
Debridement of the medial meniscus was done with use of shaver and biters. Debridement of the cartilage was also done and chondroplasty was performed with the use of a shaver. Examination of the intercondylar notch showed intact ACL.
Examination of the lateral tibiofemoral compartment showed intact cartilage and meniscus. Examination of the patellofemoral compartment showed intact trochlea, but grade 2 to grade 3 osteoarthritic lesion of the patellar cartilage.
Debridement was done with the use of a shaver. Arthroscope was inserted through the medial entry portal and shaver was reduced from the lateral entry portal to further balance the medial meniscus. Final pictures were taken and saved.
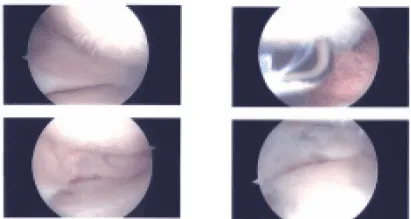
Intraoperative Images
Knee was irrigated and drained. Closure was done with # 3-0 nylon. Then 30 cc of 0.5% Marcaine mixed with 40 mg of Depo-Medrol was injected into the knee. Dressing was done with Xeroform, 4 x 8, ABD, Webril, and Ace wrap. The patient was extubated and moved to recovery in a stable condition.
The anterior cruciate, posterior cruciate, medial collateral, and lateral collateral ligaments are intact. There has been degeneration of the medial meniscus with a horizontal tear involving its body. No discrete lateral meniscal tears are present. The quadriceps and patellar tendons are intact.
The medial and lateral patellofemoral ligaments are unremarkable. A moderate knee joint effusion is present. Full thickness cartilage loss is present in the medial femorotibial compartment with associated subchondral bone marrow edema.
Less severe cartilage irregularity is present in the patellofemoral and lateral femorotibial compartments. Overall, the bone marrow signal is age-appropriate. There is no significant popliteal cyst. Popliteus muscle and tendon are intact. The iliotibial band is within normal limits. The posterior lateral corner is unremarkable.
He is status post left knee arthroscopic surgery, medial meniscectomy, chondroplasty and injection of Marcaine. He is here for his one-week postoperative visit no x rays are needed. Using crutches as he is afraid of falling. Denies fever, chills, pain is well controlled.
We have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the knee. We went over the arthroscopic pictures and removed the stitches during today’s visit. We will continue with ice and elevation of the knee to decrease swelling and pain.
We will continue to utilize early mobilization and mechanical prophylaxis to reduce the chances of a deep vein thrombosis. We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications.
We also discussed the risk and benefits and common side effects of taking these medications at today’s visit. I will see them back in three weeks’ time to evaluate their progress. With regular visits in the office, the patient did well after the surgery and continued physical therapy and rehabilitation for the knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
