The human shoulder is said to have the largest range of motion in the entire body. Our muscles in our shoulders help us to abduct, adduct, flex, extent and rotate.
According to research, rotator cuff tears, frozen shoulders, and instability are the three most prevalent injuries to the human shoulder. This article will discuss rotator cuff tears. Without treatment, rotator cuff tear may lead to permanent loss of motion.
The patient is in our office and is complaining of pain in her left foot and leg. The patient recalls becoming hurt in an automobile accident when his foot got caught between the pedals. The patient claims to have also suffered a concussion. From the foot up to the calf, there is agony.
The patient complains that it hurts to move his toes. The discomfort is very intense. Sharp pain is how the patient describes it. Constant pain might be disruptive to sleep. The patient claims he was a wrestler in the past. Bruising, tingling, and radiating pain are symptoms of the pain.
The pain is not accompanied by any of the following: swelling, numbness, weakness, abnormalities of the bowel or bladder, gait issues, giving way or limping, or problems with hand function. Since it first began, the issue has gotten progressively worse. The symptoms are improved by ice. No medication is taken by the patient.
Right and Left shoulder X Ray were presented. On the right shoulder, there were no acute fractures however there is asymmetric widening of the acromioclavicular joint of the right shoulder and for further evaluation, correlation with MRI is recommended. On the other hand, the left shoulder X Ray showed normal radiographs.
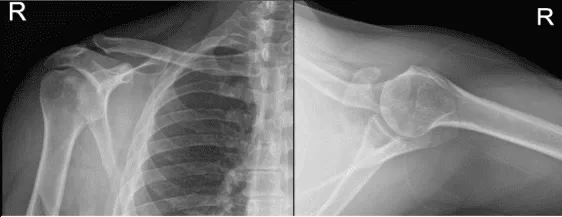
Right Shoulder X-ray
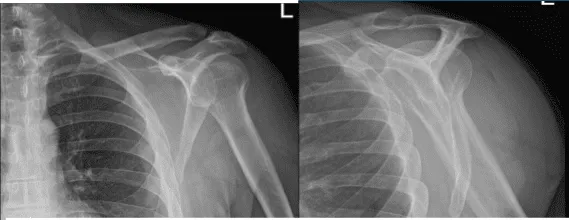
Left Shoulder X-ray
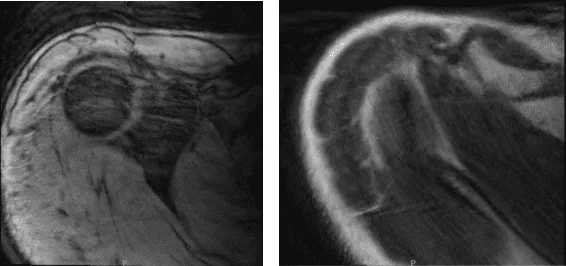
After two weeks post-operative, MRI was presented. Right shoulder MRI showed AC joint sprain and Suspected calcific tendinitis of the supraspinatus tendon.
Repeat X-ray or CT correlation is recommended for definitive assessment. Reviewed the left shoulder MRI, Focal low-grade partial tear of the anterior supraspinatus tendon and mild subacromial subdeltoid bursitis found.
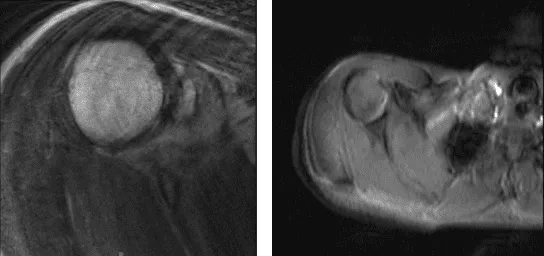
MRI-3T Right Shoulder Non-contrast
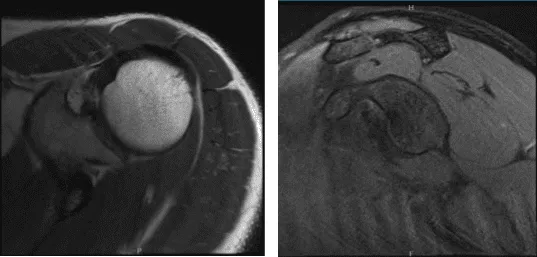
MRI-3T Left Shoulder Non-contrast
Patient decided to proceed with injection to reduce the pain and swelling regardless of the risks of it. After a sterile prep, 3cc of 1% ropivacaine, 3cc of 0.5% marcaine and 80mg of depo-medrol were injected into the left shoulder.
The patient tolerated the procedure well and there were no complications. Post injection pain, blood sugar elevation, skin discoloration, fatty atrophy and the signs of infection were discussed in detail.
After three months, the patient returned to the office still complaining of bilateral shoulder pain. Advised the patient to undergo an MRI to see any improvement from the last visit. Right Shoulder MRI still showed Chronic AC joint sprain.
MRI – 3T Right Shoulder Non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, possibility of repeat injection, possibility of shoulder pain and need for cortisone injections among others. The patient understood and signed an Informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. He was turned in the right lateral position so that the shoulder was up. The left shoulder was prepped and draped aseptically in the usual fashion.
The left shoulder was put into 40 degree of abduction and 1 0 degree of flexion. Perioperative antibiotics were given. Anterior portal was made posteriorly through a soft shoulder sport. Glenohumeral joint was reached and entry into the anterior portal was made using a spinal needle. The glenohumeral joint was examined.
Subscapularis, suprascapular, intrascapular, and biceps tendon were intact. There was no arthritic change in the glenohumeral joint. There was fraying of the glenoid labrum, which was cleaned using a shaver. There was no particular side rotator cuff tear. The scope was entered into the subacromial region. Bursitis was present.
The shaver was used to clean off the bursitis. There was some subacromial spurring which was cleaned by using bur and doing subacromial acromioplasty. The rotator cuff was examined and this was found to be Intact. Pictures were taken. There was arthritis in the AC Joint.
The decision for distal clavicular excision was taken. The distal clavicular excision was performed using the bur from the posterior portal as well as the anterior portal. A centimeter of distal clavicle was excised. Final pictures were taken and saved.
Patient returned after one-week post-operative, he is doing well, denies fever and chills. He is in a shoulder sling. After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the shoulder.
We went over the arthroscopic pictures and removed the stitches during today’s visit. We will continue with ice and elevation of the shoulder to decrease swelling and pain. We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications.
We also discussed the risk and benefits and common side effects of taking these medications at today’s visit. The patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
