The patient is a 55-year-old male presenting with complaints of wrist pain, swelling, and deformity of the left wrist. The patient had an accidental slip and fall while working in his yard and he landed with an outstretched hand on the ground. The patient initially took Tylenol and Advil for pain and did not immediately seek medical attention.
The patient has a medical history significant for major depressive disorder, migraine headaches, hypertension, and hyperlipidemia. The patient’s current medications include amlodipine, lamotrigine, sertraline, and simvastatin. The patient denies any use of illicit drugs and is a former smoker. The patient does not report any known drug allergies.

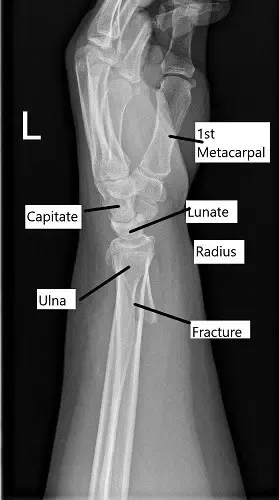
X-ray showing distal radius fracture in AP view.
The physical examination of the left upper extremity revealed swelling, warmth, and deformity of the distal forearm. There was tenderness to palpation of the radial and the ulnar styloid. The distal neurovascular examination of the left extremity was normal.
The x-ray of the left wrist revealed an oblique fracture of the distal left radius which communicates with the articular surface. There is a nondisplaced fracture of the distal left ulna. Further radiological studies in the form of CT scan revealed rotation of the distal fragment, with approximately 24 degrees of resulting apex-volar angulation.
Various treatment options were discussed with the patient at length and the patient opted for surgical management. The risks, benefits, and potential complications including infection, bleeding, nonhealing, failure of implants, need for repeat surgery, wrist arthritis, and need for rehabilitation among others were discussed with the patient. The patient understood and signed the informed consent.
X-ray showing distal radius fracture in lateral view.
PREOPERATIVE DIAGNOSIS: Displaced fracture, the distal end of radius on the left side.
POSTOPERATIVE DIAGNOSIS: Displaced fracture, the distal end of radius on the left side.
OPERATION: Open reduction and internal fixation of the distal end of radius with plate and screws.
DESCRIPTION OF PROCEDURE: The patient was taken to the operating room where she was placed on a well-padded operating room table. General anesthesia was induced. A tourniquet was applied on the left upper extremity. The splint was removed. The left upper extremity was prepped and draped aseptically in the usual fashion. Time-out was called after the preop antibiotic was given. Tourniquet was elevated.
The surgical incision was marked along with Henry’s approach. The distal one-fourth of the volar Henry approach was utilized for the incision. After the skin incision, the superficial fascia was incised along the line of the incision. With blunt dissection and achieving hemostasis using bipolar cautery, the radial artery was reached.
The radial artery was retracted laterally to find the interval between the brachioradialis and the flexor carpi radialis. The flexor carpi radialis was affected medially. The feeder vessels of the radial artery were cauterized and cut. With blunt dissection, the superior surface of the pronator quadratus was reached.
The pronator quadratus was cut along the lateral border of the radius leaving a cuff of muscle. The bone was reached and the fracture was exposed. The fracture site was opened and washed thoroughly. The fracture was reduced and clamped with a reduction clamp and a lobster clamp. The reduction was checked under C-arm and found to be acceptable.
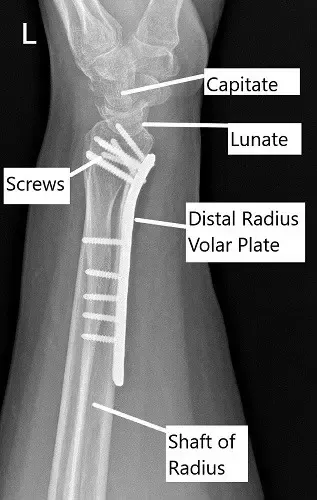
Post-operative x-ray of the wrist in lateral view.
A 5-hole distal radius plate was put and held with a radial olive wire. AP and lateral views were checked and found to be satisfactory. Provisional fixation of the plate was done with a cortical screw oblong hole. Fixation of the plate to the proximal radius was done with a nonlocking screw. Again, checking the reduction to be acceptable, the distal plate was fixed to the distal end of the radius.
A 26 mm cortical nonlocking screw was used to pull the plate to the bone. This screw was later removed and exchanged for a locking screw. The distal fixation was done using multiple locking screws. A proximal fixation of the radius was done using a combination of locking and non-locking screws. The final fixation was checked under C-arm and found to be acceptable.
The wound was thoroughly washed. Tourniquet was released. The Pronator quadratus was repaired. Hemostasis was achieved. Surgicel was put in the wound to avoid the ooze. The closure was done for the subcutaneous using Vicryl #2-0 and the skin using Monocryl #4-0.
The dressing was done using Adaptic, 4 x 8, Webril. A Longarm splint was applied in supination. The x-rays were done before completing the surgery to find that the radioulnar joint was stable and intact. We did not find the need of putting radioulnar K-wires. The patient was extubated and moved to recovery in a stable condition.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
