The painful symptoms of numerous conditions that harm the cartilage surfaces and other soft tissues surrounding the joint may be alleviated through knee arthroscopy.
The following knee arthroscopic procedures are typical: Meniscus transplanting, meniscus repair after a damaged meniscus, or partial meniscectomy. Today, we will tackle the medial and lateral meniscectomy performed to a patient experiencing pain for almost two years ago.
Patient complained of right knee pain that had started two years earlier when they visited our office. The patient said that another orthopedic surgeon had informed her that knee surgery is an option for her. The patient claims that her knee locks and clicks.
The level of discomfort is modest to severe. Aching is how the patient describes the pain. The pain is sporadic and does not interfere with sleep. She received a cortisone injection, and it has been beneficial for her.
Up until three weeks prior, the issue had been getting better, but then the discomfort returned. The symptoms are alleviated by rest, ice, physical therapy, naproxen, and Motrin. Since the prior appointment, her discomfort has not gotten any better and has really gotten worse.
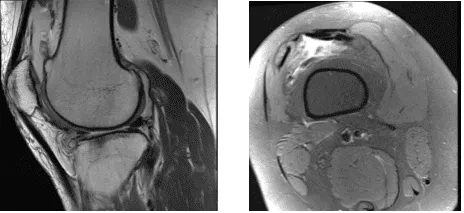
MRI were presented and found horizontal tear anterior horn and body lateral meniscus with intrasubstance meniscal cyst contiguous with the anterior 1 tear and edema in the anterior infrapatellar fat.
Lateral subluxation patella with patellofemoral arthrosis with Joint effusion with synovitis were observed. Also, her hamstring and gastrocnemius tendinopathy with medial bursitis.
We discussed treatment options and we agreed to try the conservative management for now. She will continue to attend sessions with her physical therapist, will continue to take OTC anti-inflammatory medications and decided to get another injection of cortisone.
After several weeks, the patient came back and was still complaining about her knee. We discussed treatment options and the patient opted for surgical management.
We discussed risks and benefits including infection, non-healing, repeat tear and need for surgery, injury to adjacent nerves and vessels, systemic complications like blood clots, neurological, cardiac, pulmonary complications and even death. The patient understood and signed an informed consent.
The patient was taken to the operating room where she was placed on a well-padded operating table. General anesthesia was Induced. Right lower extremity was prepped and draped with a low-thigh tourniquet aseptically in the usual fashion. Tourniquet was applied. Time-out was called.
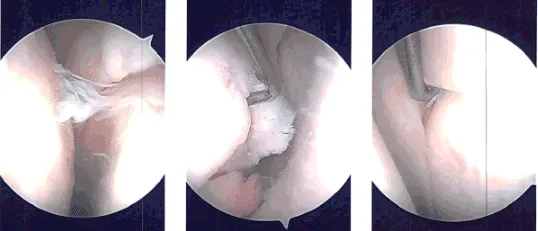
Preoperative antibiotic was already given. A lateral incision was given for the entry portal and the camera was introduced. Examination of the patellofemoral joint showed arthritic changes on the posterior surface of the patella.
Medial compartment examination showed grade 3 to grade 4 osteoarthritic changes on the medial femoral condyle as well as a tear of the anterior horn of the medial meniscus.
Medial portal was made under visualization using a spinal needle. A shaver was introduced and debridement of the anterior horn of the medial meniscus as well as the osteoarthritic lesion and abrasion chondroplasty of the medial femoral condyle was performed. A scope was entered into the intercondylar area where the ACL was found to be intact.
The scope was entered into the lateral compartment where there was diffuse fraying on the medial margin of the lateral meniscus. There was a tear of the anterior horn of the lateral meniscus also. Shaving and debridement of the lateral meniscus was performed using a shaver.
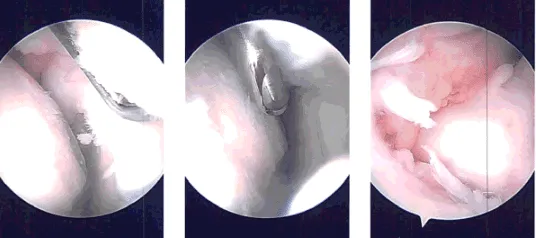
After all of shaving, the camera was introduced in the patellofemoral joint where the grade 3 to grade 4 osteoarthritic changes of the trochlea were observed and abrasion chondroplasty was performed.
There were grade 2 to grade 4 osteoarthritic changes on the posterior surface of the patella which were debrided. was performed using a shaver.
Now, the scope was entered through the medial portal and the scope was entered through the medial portal and further debridement of the lateral meniscus was performed using a shaver, upfitters, back biter and left-sided biters.
After balancing the medial aspect of the lateral meniscus, the rest of the examination was performed and the findings were taken.
The knee was irrigated. Closure was done after irrigation using # 3-0 nylon; 10 cc of 0.5% Naropin with 40 mg Depo-Medrol was injected in the knee. Tourniquet was removed.
Dressing was done using Adaptic, 4 x 4, Webril and Ace wrap. The patient was extubated and moved to recovery in stable condition.
Patient returned to the office after one-week post-operative. Her pain, bruising and swelling have improved. Denies fever and chills. For four-week post-operative check up her pain, bruising and swelling had been improving when she had a fall on both knees following which she is having pain and swelling on the right knee and abrasions on left knee.
Right knee is healing fine. In order to rehab the knee, we have chosen to combine conventional physical therapy with a home exercise program. Every three to four weeks, the patient would attend the office as usual. After the operation, the patient recovered well and kept up with physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
