By encouraging the creation of new tendon-like tissue, the Regent Bio inductive Implant aids in tendon healing. This growth makes the rotator cuff tendons thicker and aids in healing tissue damage.
The rotator cuff tendon becomes thicker as a result of the implant, which stimulates the growth of new tendinous tissue across its surface. The partial thickness tear is covered by the Regeneten patch.
After that, the rotator cuff thickens the patch by growing into the deteriorated area of the cuff. This extra thickness relieves pressure from the cuff’s degenerated area, allowing it to heal.
The patient is a 51 year-old female with right wrist and right shoulder pain that began a month ago due to a motor vehicle accident. She was suffering from right shoulder pain.
MRI showed high-grade partial rotator cuff tear along with AC arthritis, labral tear, and degenerative changes. The patient tried nonoperative treatment, but did not help.
We discussed treatment options and opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to adjacent nerves and vessels, need for repeat surgery, shoulder arthritis, and need for shoulder replacement in future, shoulder rehabilitation, among others. We also discussed the difficulty of surgery due to the patient’s weight.
We also discussed the systemic complications including cardiac, pulmonary, neurological, including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. Supraclavicular block was also given. Preop antibiotics given. The patient was put into the left lateral position with the axillary roll in place. All the bony prominences were well padded.
Bean Bag was used to place the patient in position. The right upper extremity was prepped and draped aseptically in the usual fashion. Time-out was called. Preoperative antibiotic was given.
The posterior entry portal was made, which was a soft spot. Arthroscope was entered into the glenohumeral ligament. Anterosuperior portal was also made with the use of Shaver and was introduced from the anterosuperior portal.
There was fraying of the glenoid labrum as well as articular site of the rotator cuff, which were debrided with the use of shaver. There was also partial tearing and fraying of the subscapularis tendon, which was also cleaned with the shaver.
There was no damage. Pictures were taken and saved. The arthroscope was entered into subacromial space. There was subacromial bursitis, which was debrided. There was bleeding and difficulty due to the patient’s weight and size.
Coblation wand was used followed by burr to perform acromioplasty of the right shoulder. Distal clavicle excision was also done with the use of Coblation wand and #6-0 burr. Rotator cuff was not done on the bursal site; so, a decision was made to open the rotator cuff with the use of a Regeneten implant.
Large Regeneten implant was introduced through the lateral portal and was put in place with the use of PLA tacks x8. Final pictures were taken and saved. The shoulder was thoroughly irrigated and drained.
Closure was done with the #3-0 nylon. Dressing was done with the use of Xeroform, 4 x 8, ABD, and tape. The patient was put in a shoulder immobilizer, extubated and moved to recovery in a stable condition.
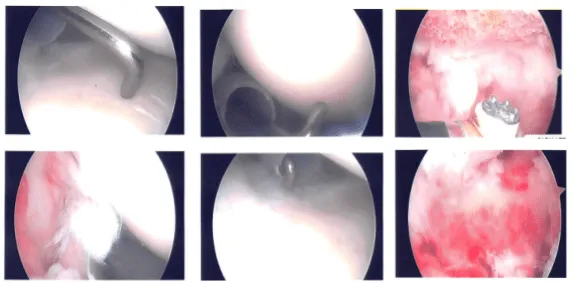
Intraoperative photo
After one week, the patient is seen in the office for her post-operative consultation, no x-rays are needed. She denies fever, chills and her pain has been improving.
After one month the patient went to the office for her monthly follow up checkup, her pain has been improving and She is without a sling and has been moving her shoulder and using it.
After discussing treatment options, we have decided to proceed with a home exercise program for rehabilitation of the shoulder. We removed the stitches during today’s visit. We will continue with ice and elevation of the shoulder to decrease swelling and pain.
We will wean them off any narcotic medications and progress to anti-inflammatories and Tylenol as long as there are no contraindications to these medications. We also discussed the risk and benefits and common side effects of taking these medications at today’s visit.
Following surgery, the patient made a full recovery and continued with physical therapy. When the patient went back for a follow-up appointment after a month, her shoulder had significantly improved.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 20, 2025.
