A meniscus root that has been ripped can be repaired surgically. Meniscal repair can be done minimally invasively using an arthroscope that is put into the knee through a tiny keyhole incision to find and repair the injured meniscus, or it can be done openly under direct vision.
Knee discomfort and swelling are two telltale indicators of a knee injury. Additionally, you could have pain when moving the joint. As you bend and straighten your leg, it could feel tight, locked up, or like it’s catching. It’s obviously cause for concern if you hear your knee pop and then give out at the moment of contact.
A 59-year-old patient visited our office with complaints regarding pain on the inner side of his right knee as well as outside of the right hip. We did the MRI of the hip and the knee, which showed medial root tear of the right knee and trochanteric bursitis of the right hip.
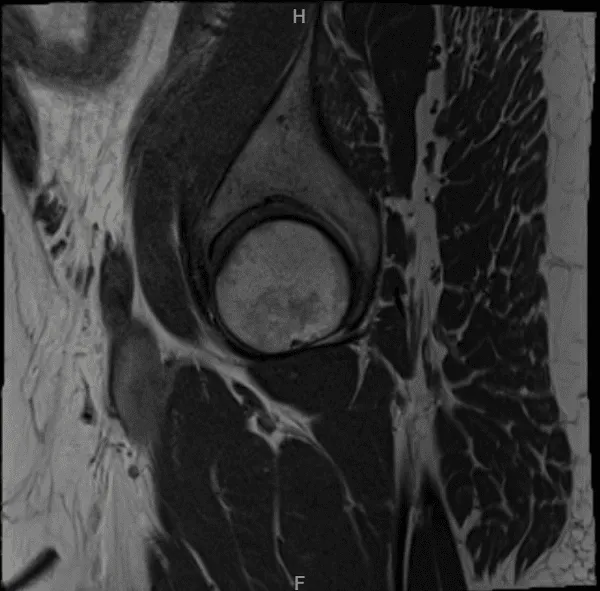
MRI Right hip non-contrast
MRI Right knee non-contrast
We discussed treatment options and the patient opted for surgical management. We discussed risks and benefits including infection, bleeding, injury to various nerves and vessels, repeat surgery, need for injections, rehabilitation, development of arthritis, and need for knee replacement in future among others. We also discussed injection of the right hip. The patient agreed and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. The patient was placed on a well-padded operating table. The right hip cortisone injection was planned at the site, which was marked before anesthesia as the most painful site.
Then, 6 mL of Marcaine 0.5% mixed with 40 mg of Depo-Medrol were injected into the area in a sterile fashion. Band-Aid was applied. A tourniquet was applied over the lower thigh.
The right knee was prepped and draped aseptically in usual fashion. The right knee was clamped in a C clamp. Preop antibiotic was given. Tourniquet was elevated after the application of Esmarch.
An anterior portal was made for a lateral arthroscopic entry portal and arthroscopic was inserted. Patellofemoral compartment showed grade 1 to grade 2 osteoarthritic changes. There was debris in the medial gutter.
Examination of the medial tibiofemoral compartment showed a tear of the medial meniscus root. A medial entry portal was made with the use of a spinal needle. Debridement of the meniscus root was confirmed and a side port insertion of the meniscus root was planned.
There was grade 1 to grade 2 osteoarthritic changes in the medial femoral condyle for which chondroplasty was performed. Examination of the intercondylar notch showed intact ACL. Examination of the lateral tibiofemoral compartment showed intact meniscus and cartilage.
Examination of the patellofemoral compartment showed grade 1 to grade 2 osteoarthritic changes, which were obtained with shaver. The planning for a medial meniscus root repair was done.
A meniscus root repair jig was inserted through the medial portal and placed at 7.5 mm anterior to the posterior mark. Flip cutter was inserted through a separate incision over the medial tibia guided by the jig. Once it was out, it was flipped and about a 5-mm tunnel was made.
Curette was further used to decorticate the bone inside the knee also. Scorpion was used to pass 2 FiberTak’s through the root, one deep and one superficial. The sutures were passed through the interosseous tunnel with the use of suture passer.
Once they were there, then the root was very well induced. The sutures were put into the tibia with the use of 4.75-mm SwiveLock and good tension was achieved, which was checked intraoperatively, and the pictures were taken and saved.
Microfracture chondroplasty was done with the use of a chondroplasty pick from Arthrex with the use of the shaver handle and 4 holes were made. The water was cut to see that there was good flow of blood from those holes.
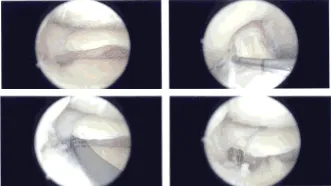
Intraoperative Arthroscopy Images
Final pictures were taken and saved. Knee was thoroughly irrigated and drained. Closure was done with the use of 3-0 nylon. Dressing was done with the use of Xeroform, 4 x 4, ABD, Webril, and Ace wrap.
A knee immobilizer was applied, which was locked in extension with the lock at 90-degree flexion. The patient was extubated and moved to Recovery in a stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. Patients regularly followed an office visit every 3-4 weeks.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
