The ulna, or forearm bone, will have holes drilled into its end by the surgeon through an incision made behind the elbow. The tendons’ ends will then be threaded through the perforations and sewn together. The tendon may be fastened to the bone by your surgeon using screws and buttons as well.
Discomfort, soreness, stiffness, and a restricted range of motion, elbow injuries and disorders can also make popping and cracking noises when moved. Additionally, you can have warmth and swelling near the joint. The joint may seem malformed in cases of elbow dislocations and fractures.
A 44 year-old patient visited our patient with complaints regarding his right arm pain due to a slip and fall on ice. He has swelling and pain in the back of the lower arm. Not able to extend the elbow. The patient reported pushing/pulling for aggravating factors.
For location, he reports right. For severity, he reports mild. He reported that the pain was associated with symptoms, he reported no weakness, no numbness, no tingling, no swelling, no redness, no warmth, no ecchymosis, no catching/locking, no popping/clicking, no buckling, no grinding, no instability, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness.
For previous surgery, he reports surgical procedure: shoulder 2006.
The patient presented an MRI results and showed complete avulsion of the posterior compartment of the distal triceps tendon with an intact anterior/deep component.
We discussed the treatment options for the patient’s diagnosis, which included living with the extremity as it is, organized exercises, medicines, injections, and surgical options. We also discussed the nature and purpose of the treatment options along with the expected risks and benefits.
I educated the patient regarding the inherent and unavoidable risks which include, but are not limited to anesthesia, infection, damage to nerves and blood vessels, blood loss, blood clots, and even death were discussed at length.
We also talked about the possibility of not being able to return to prior activities or employment, the need for future surgery, and complex regional pain syndrome. The patient also understands there is a long rehabilitative process that typically follows the surgical procedure.
We talked about the possibility of not being able to alleviate all of the discomfort. Also, I explained there is no guarantee all the function and strength will return. The patient also understands the risks of re-tear or failure to heal.
The patient expressed understanding of these risks and has elected to proceed with surgery. We have discussed the surgical procedure as well as the realistic expectations regarding the risks, outcome, and post operative protocol.
The patient was taken to the operating room where general anesthesia was induced. The right upper extremity was prepped and draped aseptically in the usual fashion. Preop antibiotic was given. A high tourniquet was applied.
A curvilinear incision was given over the olecranon along the proximal 5 cm of the forearm, around the lateral side of the olecranon extended this to about 8 cm into the distal arm over the midline.
The skin and subcutaneous tissues were cut in the line of incision. Fascia was cut in the line of incision. The bare area of olecranon was exposed and roughened with the use of rongeur. Dissection of the triceps showed a frayed and torn superficial layer.
It was dissected proximally to free it from adhesions. Insertion of SwiveLock with the FiberTape through the eyelet was planned into the olecranon in midline. A drill was inserted into the olecranon directed anteriorly and distally. Mini fluoro was used to check that there was no breach of the joint.
The drill was removed, and tap was done. The SwiveLock was inserted. The FiberWire from the SwiveLock was passed in a distal row. The two FiberTapes were passed into the proximal row. The tendon could be reduced with the elbow in about a 20-degree fraction.
The FiberWires were tied onto each other. The FiberTape was also tied onto each other. Once the knots were tied, a distal row for the suture was planned. Two SwiveLocks were used distally in the ulna on either side medial and lateral.
The three strands from either knot were into the medial and lateral ulna using the SwiveLock. The drill for the SwiveLocks was again checked for any breach of the joint. After the SwiveLocks were inserted, the sutures were cut using a sharp blade. The wound was thoroughly irrigated.
The wound was closed on each other using #0 Vicryl. The wound was closed using #0 Vicryl, # 2-0 Vicryl, # 3-0 Monocryl. The tourniquet was used only for 15 minutes and was removed because of the interaction of the triceps muscle.
Dressing was done using Xeroform, 4 x 4, Webril, posterior splint, long arm splint in 60-degree flexion and Ace wrap. Shoulder sling was applied. The patient was extubated and moved to recovery in a stable condition.
After the surgery, the patient was seen for a follow up check up and presented an X-ray result for right elbow that showed normal right elbow radiographs.
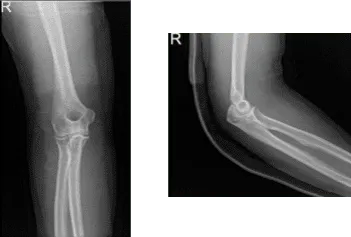
Right elbow x-ray
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the elbow.
Patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on his elbow.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
