Internal fixation is a technique for directly joining the bones. This could include specific screws, plates, rods, wires, or nails that the surgeon inserts into the bones to keep them in place. This keeps the bones from mending improperly.
The interfragmentary screw or lag screw is utilized as an adjunct to plating and is frequently employed as an initial fixation holder to ensure the safe and secure installation of a plate in a neutral mode in the reduced fracture.
The patient is a 60-year-old male who was seen in the office following a fall from the roof. He had pain and swelling of the left ankle. He was seen by another doctor and discussed treatment options including surgical and nonsurgical. But he declined surgery at that time. He was seeing another provider as a second opinion.
We reviewed x-rays and discussed treatment options and the surgical and nonsurgical treatment options. The patient opted for surgical management. The patient has recently recovered from COVID and has a history of blood clots, for which he was on Eliquis, which he has stopped recently.
We discussed risks and benefits of the surgery including infection, bleeding, nonhealing, need for repeat surgery, need for rehabilitation, blood and systemic complications including blood clots, cardiac, pulmonary, neurological complications including death. The patient understood and signed an informed consent.

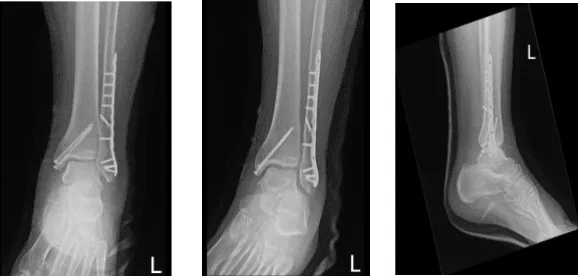
Left ankle X-ray complete 3 or more views
The patient was taken to the operating room where he was placed on a well-padded operating room table. General anesthesia was induced. The left lower extremity was prepped and draped aseptically in the usual fashion. Tourniquet was applied and inflated. Time-out was called.
Preop antibiotics were already given. A lateral incision was given centered over the fracture. The fracture was opened and washed. The fracture was reduced and fixed with the interfragmentary screw inserted. Neutralization plate was applied over the lateral malleolus with the distal and proximal screws with a combination of locking and nonlocking screws finding it in acceptable position.
Pictures were taken and saved. Now, the attention was diverted to the medial malleolus. A hockey stick incision was driven along the medial malleolus. Fracture site was reached and clean. There was a periosteum going into the fracture sites, which was excised using a blade.
The fracture was opened and washed using irrigation fluid. The fracture was reduced and held with a clamp. The two guidewires were inserted anterior and posterior to the clamp and the fracture was held in place.
Medial malleolus was performed and two malleolar screws x60 mm were inserted over the guidewires. Final tightening was done after removal of the guidewires. Pictures were taken and found to be in acceptable positions. The pictures were saved.
The wound was thoroughly irrigated and closed in layers using #0 Vicryl, # 2-0 Vicryl, and #3-0 Monocryl. Dressing was done using Xeroform, 4 x 8s, ABD, Webril.
A posterior splint was applied below the knee up to the toes with the anchor in orthostatic position and Ace wrap was applied. The tourniquet was released. The patient was extubated and recovered in the operating room only. The patient was moved to ICU once he was recovered in a stable condition.
The patient seen in the office after a week for his follow up checkup, He is in post splint and NWB. he had issues with pain control but is improving, he denies fever, chills and elevating and icing the ankle.
X rays were reviewed and discussed treatment options including PT, MRI, Injection, surgery. However, we agreed to go with conservative management for now.
Left ankle X-ray complete 3 or more views
After 2 months the patient was seen in the office for his follow up checkup, he is in post splint and NWB-PWB. He denies fever, chills, he is elevating and icing the ankle, his pain control has been improving.
And he is able to bear some weight on it. With the continued follow up checkup the patient showed progress from time to time he visits the office. He gets well after the surgery and with the help of continuing physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
