A patellar fracture is a significant injury that can make walking or straightening your knee difficult or perhaps impossible. Wearing a cast or splint while the bone heals is an effective treatment for some straightforward patellar fractures.
However, in the majority of patellar fractures, the injury causes the bone fragments to move out of position. You’ll probably require surgery if the bones are dislocated or out of alignment.
Patellar fractures that are not close to one another frequently don’t heal or heal slowly. Strong thigh muscles that connect to the patella’s top can pull the shattered fragments out of their proper positions throughout the healing process.
A 68 year-old patient was in our office with complaints post op x-rays on follow up showed cut through of the screws and failure of fixation with displacement of fracture. Dr. Karkare discussed treatment options and the patient opted for surgical management in the form of revision.
We had discussed risks, benefits, and complications including infection, bleeding, injury to adjacent nerves and vessels, possible need for repair versus partial patellectomy, repeat failure, need for rehabilitation, need for assistance in future, systemic complications including blood clot, cardia, pulmonary, cardiac, and neurological complications including death.
Dr. Karkare was also there at the time of the discussion. The patient agreed and signed an informed consent.
The patient was taken to the operating room where general anesthesia was induced. The patient was put on a well-padded operating table. Left lower extremity was prepped and draped aseptically in the usual fashion with application of tourniquet. Preop antibiotic was given. Esmarch was applied and the limb was exsanguinated and the tourniquet was elevated.
Previously, the midline incision was opened up along the same incision. Dissection was carried down deep onto the patella. A big flap of tissue was elevated on either side and retracted.
The fracture would be seen displaced with the screw tip opening out on the medially and laterally. The screws were removed with the use of a screwdriver. The fracture was thoroughly irrigated and drained. There was some crepitation of the medial side of the inferior tip of patella.
When the fracture was reduced well, it was then decided to try a tension band wiring. Two guidewires were passed medially and laterally and conversion. Findings in an acceptable position in AP and lateral view and deep enough.
Drilling was done over the guidewires and 4-mm cannulated cancellous screws were put. Both the 4-mm screws were undersized by 6 mm from measuring the guidewires. A 2-mm FiberTape was passed through these guidewires in a figure-of-eight configuration. This FiberTape showed good reduction so that the FiberWire was tied with a knot on the superolateral aspect.
The fixation was augmented with the use of 2-mm FiberTape x2 in the form of cerclage around the patella. Final fixation was achieved well. The knots were tied and buried into the tissue. The knee was thoroughly irrigated and drained.
Closure was done in layers using #0 Vicryl, #2-0 Vicryl, and staples. Dressing was done with the use of 4×8, ABD, Webril, and Ace wrap. Knee immobilizer was applied. The patient was extubated and moved to recovery in stable condition.
The patient was seen for a follow up visit and presented X-ray result that showed postsurgical changes over the patella with satisfactory position of the hardware. Otherwise, unremarkable examination.
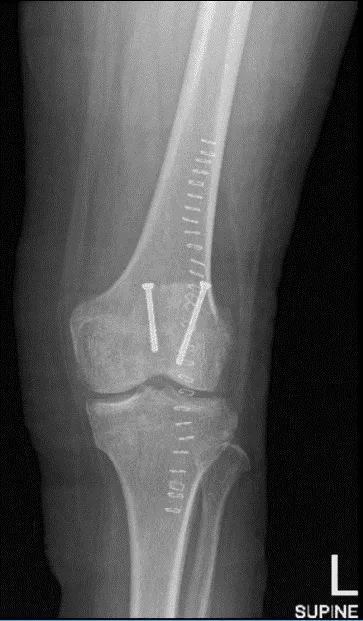
Left knee X-ray AP and Lateral
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee.
The patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on her knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 21, 2025.
