A grade 12 male student was seen in the office complaining of his injured left shoulder and neck in a vehicle accident a month ago. Patient was going to school in the school bus, sitting sideways and the bus was rear ended from the back.
He had a side-to-side swaying of his neck and head. He was seen at the hospital where CT of neck and head were done and found to be normal. Physical therapy was started by his pediatrician but he has had 2 sessions in the last week. He has had no relief in pain and has severe stiffness of the neck.
Pain affects his sleep. He is currently doing barberry which he is not able to do at present. He is taking ibuprofen at present. He also has left shoulder pain going into the front of arm associated with tingling and numbness. No gait bowel/bladder abnormality. He denies fever, chills, prior neck or shoulder pain.
Upon examination of the cervical spine, the patient is tender to palpation over the paraspinal musculature and midline from suboccipital to left shoulder blade and b/l trapezius. There is severe limitation of range of motion of the spine due to discomfort. Spurling’s test could not be done. They sit with the scapular protracted and depressed.
They are tender to palpation over the trapezius and rhomboids. They are nontender to palpation over the clavicle and elbow. There is no soft tissue swelling or ecchymosis. They have 5/5 strength, and are neurovascularly intact distally. There is no erythema, warmth, or skin lesions present.
Upon examination of the left shoulder, the patient sits with the scapula protracted and depressed. They are tender to palpation over the anterior supraspinatus and proximal biceps. There is mild palpable crepitus in the subacromial space with ranging. The patient has moderately restricted range of motion after 80-degree overhead abduction, and discomfort with above shoulder range of motion.
The patient has discomfort with impingement maneuvers Whipple testing. Stability could not be tested. They have 5/5 strength distally, and are neurovascularly intact distally. There are no erythema, warmth or skin lesions present.
X Ray of Spine and left shoulder were presented during the visit, cervical spine X-ray showed an abnormal straightening cervical curve however left shoulder showed normal radiographs. In this follow up, I advised the patient to continue taking ibuprofen and an MRI will be presented the following week.
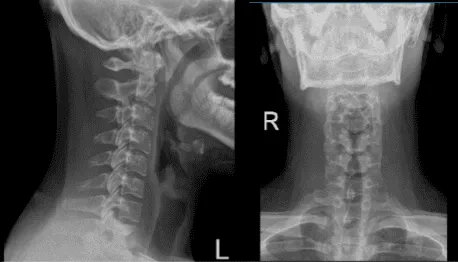
Cervical Spine X-ray 2 Views

Left shoulder X-ray
After a week patient returned with MRI result and showed that cervical spine showed significant result of straightening of the normal cervical lordosis, consistent with an element of muscle spasm and shoulder MRI showed tear of the superior glenoid labrum extending into the anchor the long head the biceps tendon.
In this scenario, advised the patient to continue the physical therapy and proceed with a pain management physician. We also discussed the surgical and non-surgical treatment for his shoulder condition.
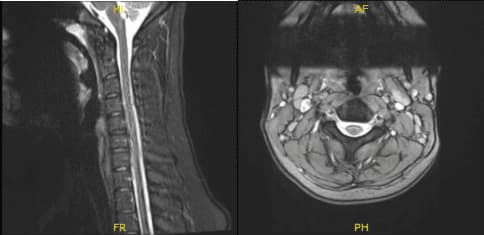
MRI-3T Cervical Spine Non-contrast

MRI-3T Arthrogram Left Shoulder
Patient decided to go with surgical treatment. We discussed treatment options and risks and benefits and complications of surgical as well as nonsurgical management.
We discussed stiffness, infection, bleeding, injury to adjacent nerves and muscles, need for repeat surgery, non-relieving of the pain, need for physical therapy. Patient and his mother understood well and signed an informed consent.
A general anesthesia induced and patient was put in lateral decubitus and position with bean bag in place. The left shoulder was prepped and draped aseptically in a usual fashion. The left arm was put into flexion and abduction on a post. Pre-draping examination under anesthesia was done and found to have no instability or subluxation.
A posterior portal, entry portal was made of the shoulder. The scope was entered into the glenohumeral joint. Examination of the glenohumeral joint was done and found to have some fraying of the articular surface of the rotator cuff as well as fraying of the anterior superior glenoid labrum and deep to the biceps tendon.
The biceps tendon was intact. The IGHL, MGHL, subscapularis, inferior and posterior labrum were intact. Pictures were taken and saved.
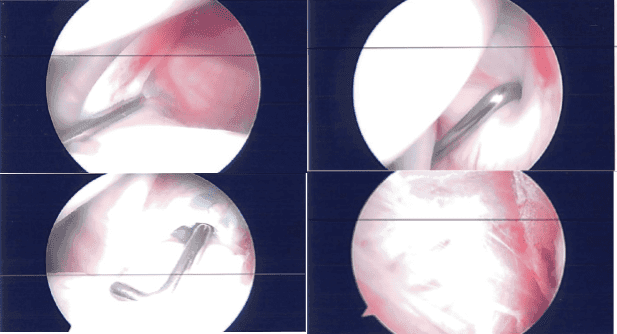
Debridement of the glenoid labrum and rotator cuff were performed using a shaver. The closure was done using nylon. Dressing was performed. The left arm was put in a shoulder sling and the patient was extubated and moved to the recovery unit in a stable condition.
After a week of seeing patients, he has been improving with regards to pain and swelling. He is limping and has been using crutches for ambulation. Denies fever, chills, reinjury. After two weeks post-surgery the incisions are healing well, without evidence of drainage, erythema or warmth.
There is a full range of motion without discomfort. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. The patient regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
