During this minimally-invasive procedure, the surgeon removes the end of the clavicle at the acromioclavicular joint in the shoulder. A rotator cuff tear may be repaired surgically using arthroscopy, open surgery, or a combination of the two.
The purpose of rotator cuff repair surgery is to reduce pain that is resistant to conventional therapies and to help the shoulder regain its flexibility and function.
The patient, a 53 year-old woman, came into my clinic complaining of both shoulder pain as a result of a car accident. She received conservative care, including physical therapy, chiropractic adjustments, and diaphoresis medicines that don’t provide much alleviation.
She was more bothered by her left shoulder than her right. We evaluated our treatment choices and chose surgery to repair the rotator cuff tendinosis, bicep tendinosis, AC arthritis, and acromioclavicular spurring of the left shoulder.
We examined the risks and advantages of surgical care, including those related to infection, bleeding, injury to nearby nerves and vessels, the need for repair, arthritis and the necessity for future shoulder replacement surgery, blood clot, cardiac arrhythmia, neurological, the patient understands and has provided informed consent, which may include death.
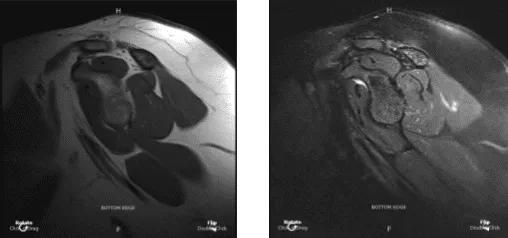
MRI Right shoulder non-contrast
The operation room, where the patient was taken, put on a surgical table with plenty of padding. Anesthesia was induced throughout. The anesthetic staff had already administered a supraclavicular block. 1g of TXA and a preoperational antibiotic were administered.
The patient’s left shoulder was placed in the right lateral position up. In the beanbag, positioning was maintained. Each bony protrusion had thick padding. The axilla received an axillary pad. A timeout was ordered. The left shoulder was prepared as normal and wrapped aseptically.
There was a cut made on the glenohumeral joint’s soft spot. Using a spinal needle, anterosuperior and anterolateral portals were created. Pictures were initially taken after the shaver and scope were introduced through the radial gateway.
The absence injury to the subscapularis, the glenohumeral cartilage, and the anterior labrum had a partial rip, which was cleaned up with a razor. The supraspinatus had partial articular sided fraying in the rotator cuff, which was cleaned up using the shaver.
The scope was placed inside of the shaver and using the anterior portal, a bursectomy was carried out in the subacromial area. The bursectomy was finished with the creation of a lateral portal. There was some acromial spurring and fraying, which was debrided with a Coblation wand followed by 6.1mm ” with burr AC acromioplasty.
Arthritis was also present, which was also debrided and this resection was done with the use of Coblation wand followed by #6-0 burr from the posterior and anterior superior portal. There was AC partial tearing in the supraspinatus tendon.
Plan was done to repair the tearing with the rotator cuff degenerative implant. The medium-sized implant was introduced through the lateral portal. PLA tacks were introduced through a separate superior” portal Good repair was achieved with the use of 8 tacks.
The shoulder was thoroughly irrigated and drained. Final pictures were taken and saved. Closure was done with the use of #3-0 nylon. Dressing was done with the use of Adaptic, 4 x 8, ABD, Webril, tape. The patient was put on shoulder immobilizer and extubated and moved to recovery in stable condition.
After the two weeks the patient was seen today for her post-operative visits, she denies fever and chills. She still has pain and needs more pain pills and she may need right shoulder scope in future.
After discussing treatment options, we have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the shoulder. We went over the arthroscopic pictures and removed the stitches during the visit.
We will continue with ice and elevation of the shoulder to decrease swelling and pain. We will wean them off any narcotic medications and progress to anti-inflammatories and
Tylenol as long as there are no contraindications to these medications. We also discussed the risk and benefits and common side effects of taking these medications. The patient will be back in three weeks’ time to evaluate their progress.
Another two weeks have passed, the patient seen in the office for her follow up checkup, she has no fever and chills, her pain is improving and she is working with Caring hands for PT.
We discussed treatment options including PT, MRI, Injection, surgery and We agreed to go with conservative management for now, PT is to continue, WBAT, Ice/heat, Elevation and taking OTC anti-inflammatory meds.
Follow Ups after 4 weeks. With continued regular checkups and attending physical therapy, the patient did well after surgery.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 24, 2025.
