Following a car accident, the following are common types of knee injuries: Fracture of the Knee: A direct strike to the kneecap from your steering wheel or dashboard may result in a fracture. The bones around your kneecap, on the other hand, can break.
Bones may crack or break cleanly, scattering shards about your knee. If you have a mild knee injury from a car accident, your doctor will most likely recommend RICE therapy, which stands for rest, ice, compression, and elevation. But in instance, sometimes RICE Therapy is not working with everyone and may lead to surgical treatment.
Patient is a 49 year-old female, in our office with complaints of LS spine and right knee pain. He experienced the pain about 8 months ago. The patient remembers his injury in a motor vehicle accident. The pain is extremely severe in intensity. The patient describes the pain as sharp, dull, stabbing.
The pain is constant and does disturb sleep. The pain is associated with swelling, bruising, radiating pain, weakness, gait problem, or limping, giving way. The pain is not associated with numbness, tingling, bowel or bladder abnormality, hand function difficulty. The problem has been getting worse since it started.
Walking, standing, lifting, exercise, twisting, lying in bed, and bending make the symptoms worse. Nothing makes the symptoms better. The patient has not undergone surgery for the same in the past. She has had cortisone injections to the back but not recently.
She presented her old X-ray done 8 months ago and suspected to have a medial meniscus tear of right knee. Suggested to take another X-ray/MRI to see the reason behind the pain. This time the patient agreed to take Cortisone injection to ease the pain somehow.

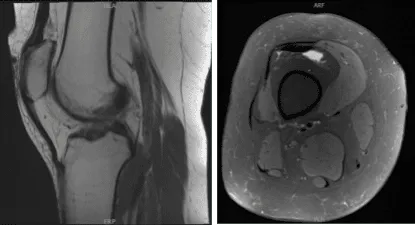
MRI of right knee
Patient returned and presented her MRI- found Tri compartment degenerative chest, with cartilage loss most pronounced in the patellofemoral compartment.
Complex tear involving the anterior horn lateral meniscus with a horizontal component extending into the body lateral meniscus with small joint effusion.
We have tried conservative management
We have tried conservative management, but it failed. We discussed treatment options and the patient opted for surgical management.
We discussed risks and benefits including infection, bleeding, nonunion, need for repeat surgery, blood clots, injury to adjacent nerves and vessels, rehabilitation, knee stiffness, need for cortisone injection and joint replacement in the future.
Risks, benefits, and complications including blood clots, cardiac, neurological, pulmonary complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where she was placed on a well-padded operating room table. General anesthesia was induced and LMA was then started. The right lower extremity was prepped and draped aseptically in the usual fashion with a low thigh tourniquet. A time-out was called.
Pre antibiotics were already given. Lateral entry portal was made through the lateral incision. The arthroscope was entered and the knee was examined. It showed a tear in the anterior horn of the lateral meniscus.
A medial entry portal was made with the use of a spinal needle with good access to the lateral compartment. The incision was given medially. A shaver was Introduced and cleaning of the synovectomy of the knee was performed.
The medial meniscus was examined using a probe. It was found to be Intact. There was no osteochondral lesion on the posterior femoral condyle. The ACL was examined and found to be intact.
On examination of the lateral compartment, there was a tear on the anterior horn of the lateral meniscus with part of the root Intact. Incision and debridement of the anterior horn was not taken as the wound was frayed.
Debridement was done using punches as well as shaver. A balanced margin was made. There was no osteochondral lesion on the lateral femoral condyle.
Upon examination of the lateral femoral condyle, there was grade 2 to grade 4 osteochondral lesions over the trochlea and the patella. Debridement of the osteochondral lesion was done using a shaver.
Chondral pick was used to do microfracture on the osseous surface of the patella at two points. The knee was thoroughly irrigated. Examination was again performed from the medial portal and balancing of the lateral meniscus was performed and confirmed.
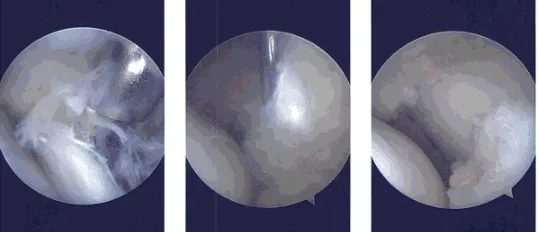
Intraoperative Arthroscopy Images
The knee was irrigated thoroughly and drained. The wound was closed using #3-0 Nylon, 0.5% lidocaine was injected to the knee. The closure was performed as well as dressing and the patient was moved to the recovery unit.
After a week of seeing patients, he has been improving with regards to pain and swelling. He is limping and has been using crutches for ambulation. Denies fever, chills, reinjury. After two weeks post-surgery the incisions are healing well, without evidence of drainage, erythema or warmth.
There is a full range of motion without discomfort. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the knee. Patients regularly followed an office visit every 3-4 weeks. Patient did well after the surgery and continued physical therapy.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
