Human biceps are the one of the three muscles used to move or to work the forearm. We used our biceps in our everyday lives especially for someone whose work requires lifting, carrying and pushing.
A 41-year-old male patient was seen in the office with complaints of having spasms in his left arm. He is currently working as a compounder. His lap coat got caught in the valve handle. He went to grab it and he felt a pop in his left shoulder. Patient states he cannot make a fist or turn arm.
The pain is extremely severe in intensity. The pain is constant and does disturb in sleep and it was associated with numbness but not associated with swelling, bruising, tingling, radiating pain, weakness, bowel or bladder abnormality, gait problem, giving way, or limping, hand function difficulty. The problem has been getting worse since it started. Nothing makes the symptoms better.
MRI results were presented and reviewed by the doctor. It showed that there is traction cyst in the greater tuberosity. There is a complete tear of the distal biceps’ tendon with tendon retraction to the level of the radial capitellum joint line with fluid along the course.
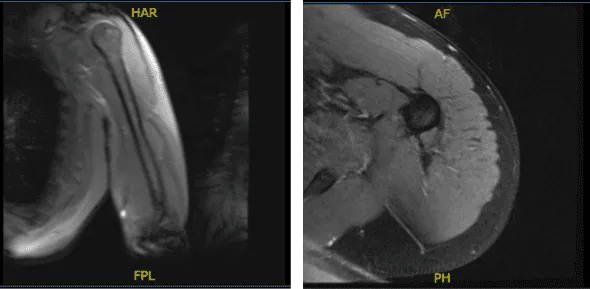
MRI-3T Left Arm Non-contrast
We discussed treatment options including surgical and non-surgical. We discussed risks, benefits, and complications of either treatment. The patient opted for surgical management.
We discussed infection, bleeding, elbow stiffness, rehabilitation, injury to adjacent nerves and vessels, re-rupture and re-repair. The patient agreed and signed an informed consent.
The patient was taken to the operating room where he was placed on a well-padded operating table. General anesthesia was induced. The left arm was put in a high a tourniquet followed by usual aseptic prep and draping. A time-out was called. Tourniquet was elevated after exsanguination.
An incision was given about 3 cm distal to the elbow crease line. A transverse incision of about 5 cm in length. With sharp and blunt dissection, the medial border of the brachioradialis nerve was reached. The lateral antebrachial cutaneous nerve was seen and dissected free and retracted gently on the lateral side.
Biceps Aponeurosis could be seen and tacked on to the biceps stump, which was folded up to itself and stuck to the surrounding tissue. The stump was released with sharp and blunt dissection and delivered out of the wound. The stump was prepared using #2 Fiber Loop with whipstitch sutures.
Now, the radial tuberosity was exposed using a periosteal elevator and retracted. A 3.2 drill bit was passed bi-cortically and checked under C-arm and found to be over radial tuberosity.
8mm Acorn reamer was used to ream the single cortex of the radius at the level of the neck. The biceps tendon stump was 7 in diameter. Now, the button was loaded and put on the inserter and passed through both cortices of the radius.
A curved needle was taken and one limb of the suture was passed through the tendon and a knot was tied. Now, the other limb was passed through the screwdriver using a wire passer.
The screw was brought on to the radial side of the uni-cortical hole and finally tightened flush with the bone. The wound was thoroughly washed and the tourniquet was removed.
Closure of the wound was done using Vicryl #2-0 and Monocryl #4-0. Dressing using 4 x 4s, ABD, Webril, and Ace wrap was done. The patient was extubated and moved to the recovery unit.
After 1 week of operation, the patient was seen in the office. He had a lot of pain after the surgery and was given a brachial block. Pain has been getting better.
He is able to move his elbow gently. Denies fever, chills. He does complain of numbness along the lateral aspect of the forearm. He is able to move well at his shoulder, wrist, fingers and thumb.
After a month, the postoperative patient returned to the office. On examination of the contralateral extremity, the patient is nontender to palpation and has excellent range of motion, stability and strength.
After 12 weeks from the operation, he has been getting better. He is able to move his elbow freely. He lifts 25lbs 10 sets of 10 every day.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
