Raising your arm is difficult and painful. When you move your arm, you may hear or feel popping or clicking. shoulder discomfort that becomes worse at night or when you rest your arm.
Reattaching the rotator cuff tendon to the humeral head is the most common surgical procedure used to treat a torn rotator cuff. However, a partial tear might only require debridement, or trimming or smoothing procedure. The tendon is stitched back to its original location on the humerus to heal a full rip.
A 29 year-old patient was in our office with complaints regarding right shoulder and b/l knee pain due to a motor vehicle accident. For aggravating factors, patients reported standing, walking, twisting, and weightbearing.
For associated symptoms, weakness, warmth, catching/locking, popping/clicking, buckling, grinding, tender to the touch, and pain with motion but reported no numbness, no tingling, no swelling, no redness, no ecchymosis, no instability, no radiation, no drainage, no fever, no chills, no weight loss, and no change in bowel/bladder habits. Patient did not have pain in these body parts before the current injury.
The patient presented MRI results of left shoulders that showed Moderate grade partial-thickness bursal surface tear of the distal supraspinatus tendon with accompanying subacromial subdeltoid bursitis.
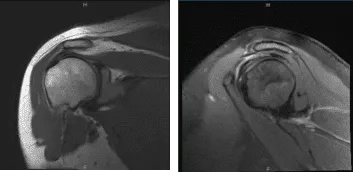
MRI-3T Left Shoulder non-contrast
We discussed treatment options and opted for surgical management. We discussed risks and benefits Including infection, bleeding, injury to adjacent nerves and vessels, need for rehabilitation, need for repeat surgery, continuation of shoulder pain, systemic complications including cardiac, pulmonary, and neurological complications including death.
The patient understood and signed an informed consent.
The patient was given a supraclavicular block in the holding area. The patient was taken to the operating room where she was placed on a well-padded operating room table. General anesthesia was given. Preoperative antibiotics in the form of 2 g of Ancef was given. Tranexamic acid 1 g was also given.
The patient was turned into a right lateral position with the left shoulder up. All the bony prominences were well padded. The patient was held in a position in a beanbag. Left shoulder was prepped and draped aseptically in the usual fashion soft spot. An arthroscope was inserted.
Anterosuperior portal was made with the use of a spinal needle. Shaver and probe were inserted from the anterosuperior portal. Examination of the glenohumeral joint showed intact cartilages, Intact rotator cuff, intact scapula, intact labrum, and intact biceps. The examination was normal.
The arthroscope was removed and re-inserted into the subacromial space. A shaver was introduced from the anterosuperior portal. A Bursectomy was performed. Examination of the rotator cuff showed a partial rotator cuff tear on the bursal side. There was no fraying of the acromion.
The AC joint did not show any arthritis. Decision was taken not to do distal clavicle excision. The plane of the rotator cuff tear was implanted. Lateral entry anterior portal was made. We completed the bursectomy.
The implant was introduced from the lateral portal and seemed to cover the rotator cuff tear. A separate portal was made to pass the tracks. A sleeve was inserted followed by multiple tacks to hold the implant in place.
The handle was removed. The lateral part of the implant was fixed to the bone with the use of bone anchors x2. Final pictures were taken and saved.
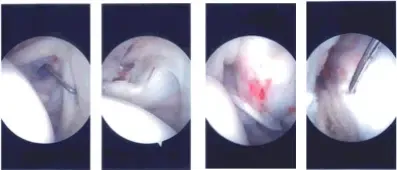
Intraoperative Arthroscopy Images
The shoulder was thoroughly irrigated and drained. Closure was done with #4-0 nylon. Dressing was done with the use of Adaptic, 4 x 8, ABD, and tape. Shoulder immobilizer was then applied. The patient was extubated and moved to the recovery unit in a stable condition.
The patient was seen for post operative check up. We have decided to do formal physical therapy as well as a home exercise program for rehabilitation of the shoulder.
The patient did well after the surgery and continued physical therapy. Patient checked in for a follow up visit after a month and saw significant improvement on her shoulder.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 19, 2025.
