Knee arthroscopy can help with a variety of conditions that hurt the soft tissues around the joint and the cartilage surfaces. Meniscus repair, and meniscus transplanting are among the common arthroscopic operations for the knee.
Some individuals believe that meniscus tears will naturally heal with time. However, the fact is that there are various meniscus rips, and certain tears cannot heal on their own. If your meniscus tear is on the outside third of the meniscus, it could mend naturally or need to be surgically fixed.
A 68 year-old patient has been in our office with complaints of right knee and right shoulder pain since approximately August 2020. She is currently retired. She has swelling of both calf and knee.
For aggravating factors, patients report walking, lifting, and twisting. For associated symptoms, she reports swelling, popping/clicking, buckling, instability, and pain with motion but reports no weakness, no numbness, no tingling, no redness, no warmth, no catching/locking, no radiation, no drainage, no fever, no chills, no weight loss, no change in bowel/bladder habits, and no tenderness.
For location, she reports right. For quality, she reports sharp, constant, and worsening. For severity, she reports severe.
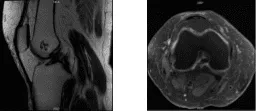
She presented an MRI result for right knee and there was a tear and degeneration with moderate loss of substance of posterior lateral aspect of lateral meniscus, detachment of posterior horn from tibial insertion and tear at anterolateral aspect.
Small shallow inferior surface partial tear of posterior horn of medial meniscus. Mild chondromalacia of the patella. Moderate lateral compartment degenerative disease predominantly posterior lateral aspect. Joint effusion. Benign enchondroma in distal femur.
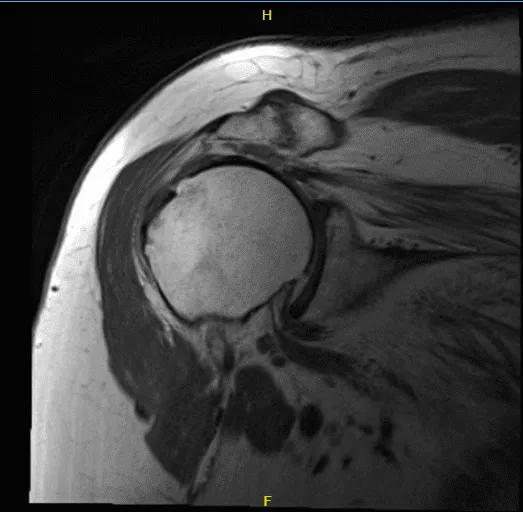
For MRI right shoulder, large full-thickness tear of supraspinatus tendon. Tear excluding its posterior tendon that is partially torn. There is moderate muscle. Partial tear of infraspinatus tendon. Complete tear of subscapularis tendon that is scarred to the capsule associated with near complete muscle atrophy.
Medial dislocation of long headed biceps tendon with tendinosis and partial tear. Mild glenohumeral and moderate acromioclavicular joint degenerative disease. Moderate subacromial subdeltoid bursitis.
MRI-3T Right knee non-contrast
MRI-3T right shoulder non-contrast

Doppler Venous Lower Extremity Bilateral
The doppler venous lower extremity results have shown no sonographic evidence for lower extremity deep or superficial venous thrombosis bilaterally. We discussed treatment options and considering the root tear, we opted for surgical management.
We discussed the risks and benefits including infection, bleeding, nonhealing, need for re-repair, need for replacement, need for rehabilitation in the future. We also discussed systemic complications including blood clots, cardiac, pulmonary, neurological complications including death. The patient understood and signed an informed consent.
The patient was taken to the operating room where she was placed on a well-padded operating room table. General anesthesia was induced. A tourniquet was applied on the lower thigh. Preoperative antibiotics were already given. The tourniquet was inflated. A lateral entry portal was made for examination.
The arthroscope was inserted. Examination showed some fraying of the lateral margin, inner margin of the medial meniscus. The margins were shaved and a bitter was used to balance the margins. There was no significant chondral damage to the medial compartment.
The arthroscope was entered into the intercondylar notch where it showed an ACL with mild degeneration. The ACL was intact. The arthroscope was entered into the lateral compartment where we could see a lateral meniscus tear along the posterior horn with fraying and degeneration. The posterior root was intact. Shaver and upbitters were used to balance the meniscus to stable margins.
The lateral meniscus was loose in the popliteal hiatus, but it was decided not to excise it considering that it was not mobile enough to come into the joint. Examination of the patellofemoral joint showed grade 2 to grade 3 osteoarthritic lesions of the inferior of the posterior surface of the patella. There was no chondral damage on the trochlea. Chondral shavings were done. Final pictures were taken and saved.

Intraoperative Arthroscopic Images
The knee was irrigated and drained. Closure was done using #3-0 nylon. Then 40 mg of Depo-Medrol mixed with 9 cc of Naropin was injected into the knee. Dressing was done using Adaptic, 4 x 8, ABD, Ace wrap, and Webril. The patient was moved to recover in a stable condition.
We have decided to proceed with formal physical therapy as well as a home exercise program for rehabilitation of the knee. The patient did well after the surgery and continued physical therapy. The patient checked in for a follow up visit after a month and saw significant improvement in her knee.
Disclaimer – Patient’s name, age, sex, dates, events have been changed or modified to protect patient privacy.
The content on this page has been authored, edited, or approved by the doctors below, and was last reviewed for accuracy on October 18, 2025.
